Department of Neuroscience, University of Turin, Turin, Italy.
Clinical Psychology Unit, "Città Della Salute E Della Scienza Di Torino" Hospital of Turin, Turin, Italy.
Neurol Sci. 2022 Jul;43(7):4107-4124. doi: 10.1007/s10072-022-06068-x. Epub 2022 Apr 23.
To explore the pathogenetic hypothesis provided to explain the comorbidity of anxious and depressive symptomatology and AD and to assess the association between anxious and depressive symptoms and the AD-related cognitive impairment.
In October 2020 and March 2021, PsycINFO, Embase, Ovid, and CINAHL were searched for peer-reviewed original articles investigating anxiety and/or depression in AD.
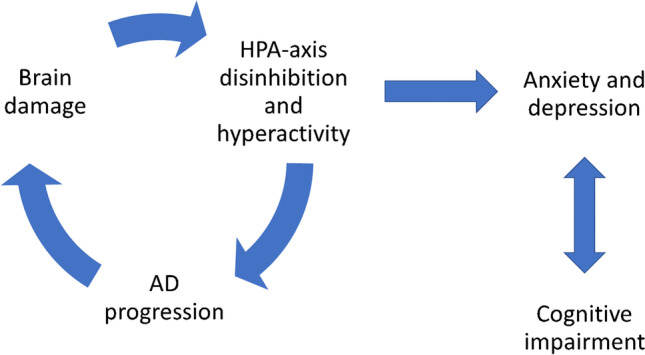
A total of 14,760 studies were identified and 34 papers on AD patients were included in the review. Suggested biological causes of depression and anxiety in AD include higher strychnine-sensitive glycine receptor (GlyRS) functioning and selective reduction of N-methyl-D-aspartate (NMDA) receptor NR2A density, cortical and limbic atrophy, lower resting cortical metabolism, lower CSF Aβ42 and higher t-tau and p-tau levels, and neuritic plaques. At the same time, dysthymia arises in the early stages of AD as an emotional reaction to the progressive cognitive decline and can cause it; anxiety can appear as an initial compensating behaviour; and depression might be related to AD awareness and loss of functional abilities. Affective symptoms and the expression of the depressive symptoms tend to reduce as AD progresses.
The neurodegeneration of areas and circuits dealing with emotions can elicit anxiety and depression in AD. In the early stages of the disease, anxiety and depression could arise as a psychological reaction to AD and due to coping difficulties. In late AD stages, the cognitive impairment reduces the emotional responses and their expression. Anxiety and depression are more intense in early-onset AD, due to the major impact of AD on the individual.
探索解释焦虑和抑郁症状与 AD 共病的发病假说,并评估焦虑和抑郁症状与 AD 相关认知障碍的相关性。
2020 年 10 月和 2021 年 3 月,在 PsycINFO、Embase、Ovid 和 CINAHL 上搜索了探讨 AD 中焦虑和/或抑郁的同行评议原始文章。
共确定了 14760 项研究,综述纳入了 34 篇关于 AD 患者的论文。AD 中抑郁和焦虑的潜在生物学原因包括更高的苦毒敏感甘氨酸受体(GlyRS)功能和 NMDA 受体 NR2A 密度的选择性降低、皮质和边缘萎缩、静息皮质代谢降低、CSF Aβ42 降低和 t-tau 和 p-tau 水平升高,以及神经原纤维缠结。同时,心境恶劣在 AD 的早期阶段出现,作为对进行性认知下降的情绪反应,并可能导致认知下降;焦虑可能表现为初始代偿行为;抑郁可能与 AD 意识和功能丧失有关。随着 AD 的进展,情绪症状和抑郁症状的表达往往会减少。
与情绪处理相关的区域和回路的神经退行性变可引发 AD 中的焦虑和抑郁。在疾病的早期阶段,焦虑和抑郁可能是 AD 的心理反应和应对困难引起的。在 AD 晚期,认知障碍降低了情绪反应和表达。早发性 AD 中的焦虑和抑郁更为强烈,因为 AD 对个体的影响更大。