Vullo P A, Olivera Moreno D, Crego Vita D
Department of Anaesthesia, Critical Care and Pain Unit, Hospital Central de la Defensa Gómez Ulla-IMIDEF, Glorieta del Ejército #1, Madrid, Spain.
Department of Anaesthesia, Critical Care and Pain Unit, Hospital Central de la Defensa Gómez Ulla-IMIDEF, Glorieta del Ejército #1, Madrid, Spain.
Int J Surg Case Rep. 2022 May;94:107033. doi: 10.1016/j.ijscr.2022.107033. Epub 2022 Apr 6.
Metallosis is produced by friction between prothesis pieces, release of metal particles that can enter systemic circulation provoking cobalt or chromium poisoning. No studies have been found in which the mobilization of metal particles causes haemodynamic instability.
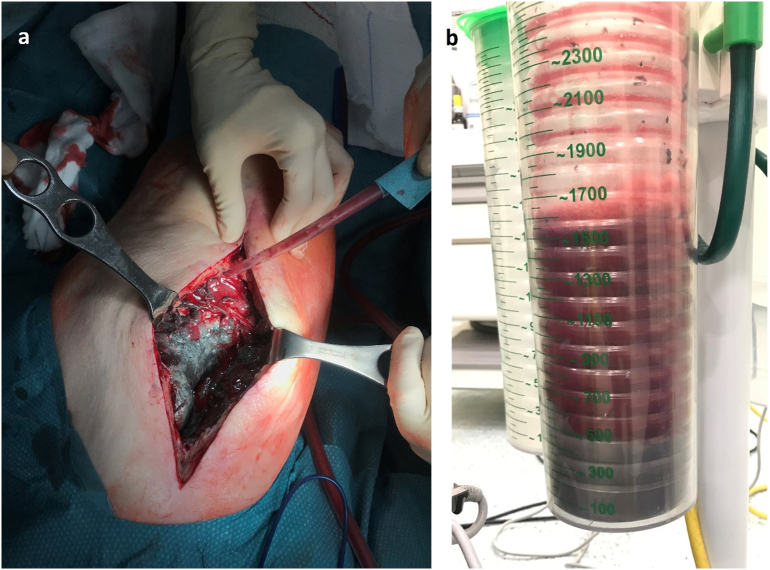
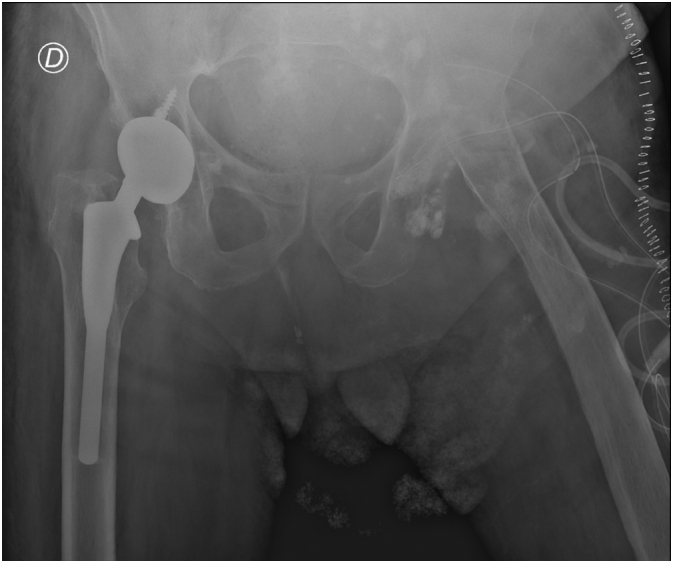
We present the case of an 85 years old male with metallosis, programmed for washing and prothesis extraction (Girldlestone procedure). During pseudotumor drainage and washing, patient presented sudden desaturation and hypotension refractory to volume and phenylephrine administration. Echocardiogram showed overall hypocontractility. Situation was controlled with high inspired oxygen fraction and noradrenaline perfusion. In postoperative period E. coli grew in pseudotumor samples and metal particles could be seen in soft parts as the testicles. Plasma metal concentration showed high levels of chromium, but no chelator treatment was needed.
Intraoperative hypotension raises several differential diagnoses. Echocardiography was useful to rule out hypovolaemia, pulmonary embolism and cardiac ischaemia. The results of analytical tests are often delayed, especially cultures and plasma metal levels; therefore, if metal poisoning is suspected, supportive treatment should be performed. Chelation and plasmapheresis should be used once the diagnosis is certain and are therefore not useful in the acute phase.
Intraoperative hemodynamic instability during hip prosthesis explant may be due to bleeding, release of inflammatory or infectious detritus, acute pulmonary thromboembolism, etc. However, the sudden increase of cobalt or chromium ions should be considered as a feasible option in patients with metallosis, despite not presenting previous clinical manifestations of intoxication.
金属沉着病是由假体部件之间的摩擦产生的,金属颗粒的释放可进入体循环,引发钴或铬中毒。尚未发现有研究表明金属颗粒的移动会导致血流动力学不稳定。
我们报告一例85岁患有金属沉着病的男性患者,计划进行冲洗和假体取出术(Girldlestone手术)。在假瘤引流和冲洗过程中,患者突然出现低氧血症和低血压,对液体输注和去氧肾上腺素治疗无效。超声心动图显示整体心肌收缩力下降。通过高吸氧浓度和去甲肾上腺素灌注控制了病情。术后,假瘤样本中培养出大肠杆菌,在软组织如睾丸中可见金属颗粒。血浆金属浓度显示铬水平升高,但无需螯合剂治疗。
术中低血压引发了多种鉴别诊断。超声心动图有助于排除低血容量、肺栓塞和心肌缺血。分析测试结果往往延迟,尤其是培养结果和血浆金属水平;因此,如果怀疑金属中毒,应进行支持性治疗。一旦确诊,应使用螯合疗法和血浆置换,因此在急性期无效。
髋关节假体取出术中的血流动力学不稳定可能是由于出血、炎性或感染性碎屑释放、急性肺血栓栓塞等原因。然而,对于患有金属沉着病的患者,尽管之前没有中毒的临床表现,但钴或铬离子的突然增加应被视为一种可能的情况。