Department of Obstetrics and Gynecology, Oslo University Hospital, Oslo, Norway.
Faculty of Medicine, University of Oslo, Oslo, Norway.
Acta Obstet Gynecol Scand. 2022 Jul;101(7):794-802. doi: 10.1111/aogs.14363. Epub 2022 Apr 25.
Beta-blockers are prescribed for many pregnant women with heart disease, but whether there is a dose-dependent effect on fetal growth remains to be examined. We aimed to investigate if antenatal beta-blocker use and dose were associated with delivering a small-for-gestational-age infant among women with heart disease.
Our cohort included women with heart disease who delivered at Oslo University Hospital between 2006 and 2015. Maternal heart disease was classified into modified WHO risk scores. Women with beta-blocker treatment were dichotomized into whether they had been treated with a low or high dose based on clinical factors. We compared the risk of delivering a small-for-gestational-age infant in women exposed to high doses, low doses, or with no exposure to antenatal beta-blockers while adjusting for severity of maternal heart disease in logistic regression models.
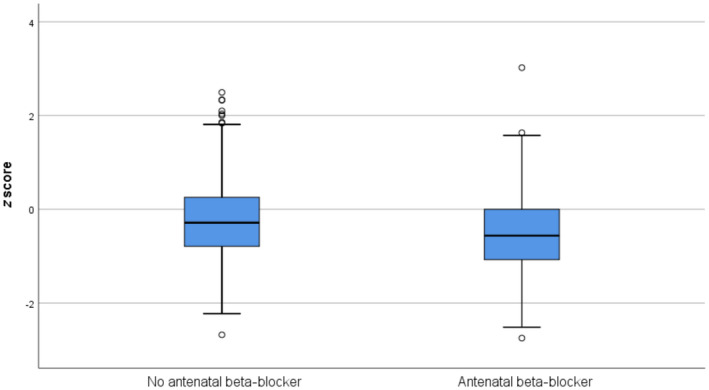
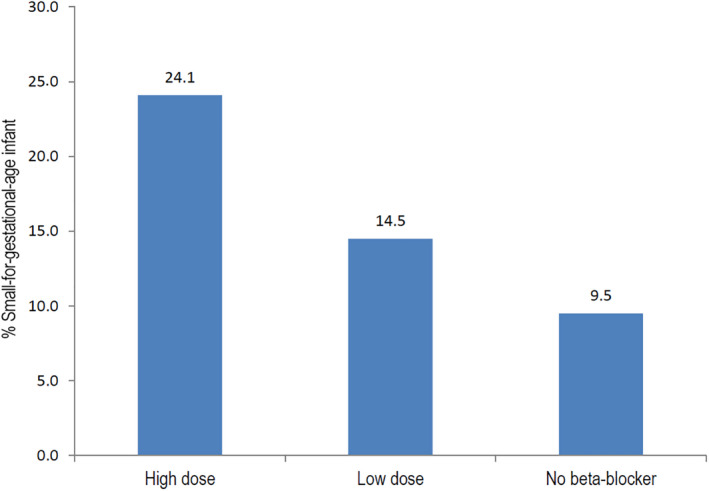
Of a total of 540 pregnancies among women with heart disease, 163 (30.2%) were exposed to beta-blocker treatment. The majority were treated with metoprolol (86.5%). Almost twice as many babies in the beta-blocker group were small-for-gestational-age, compared with the non-exposed group (19.8 vs 9.5%, P < 0.001). Women using a high-dose beta-blocker had a five-fold increased risk of delivering a small-for-gestational-age infant compared with non-exposure (adjusted odds ratio [aOR] 4.89, 95% confidence interval [CI] 2.22-10.78, P < 0.001). Women using a low dose of beta-blocker had a two-fold increased risk of delivering a small-for-gestational-age infant; however, the confidence interval included the null (aOR 1.75, 95% CI 0.83-3.72, P = 0.143). Results when restricting the analyses to metoprolol showed the same pattern, but with attenuation of risks.
We found a five-fold increased risk of delivering a small-for-gestational-age infant in women with heart disease treated with a high dose of beta-blocker, and a two-fold increased risk among those treated with a low dose, showing an apparent dose-response relation. Close monitoring of fetal growth is warranted among women with heart disease treated with beta-blockers. As drug therapy in pregnancy concerns both mother and fetus, an optimum balance for both should be the goal.
β受体阻滞剂被广泛用于治疗患有心脏病的孕妇,但目前仍不清楚其剂量是否与胎儿生长受限有关。本研究旨在探讨患有心脏病的孕妇使用产前β受体阻滞剂及其剂量与小于胎龄儿(SGA)发生的关系。
本队列纳入了 2006 年至 2015 年期间在奥斯陆大学医院分娩的患有心脏病的孕妇。根据改良的世界卫生组织(WHO)危险评分对产妇心脏病进行分类。根据临床因素,将接受β受体阻滞剂治疗的患者分为低剂量和高剂量组。通过逻辑回归模型,在校正母亲心脏病严重程度后,比较高剂量、低剂量或未暴露于产前β受体阻滞剂的孕妇发生 SGA 儿的风险。
在患有心脏病的 540 例妊娠中,163 例(30.2%)接受了β受体阻滞剂治疗。其中,美托洛尔的使用率最高(86.5%)。与未暴露组相比,β受体阻滞剂组的 SGA 儿发生率几乎高出一倍(19.8%比 9.5%,P<0.001)。与未暴露相比,使用高剂量β受体阻滞剂的孕妇发生 SGA 儿的风险增加了五倍(调整后的比值比[OR] 4.89,95%置信区间[CI] 2.22-10.78,P<0.001)。使用低剂量β受体阻滞剂的孕妇发生 SGA 儿的风险增加了两倍;然而,置信区间包含了无效值(调整后的 OR 1.75,95%CI 0.83-3.72,P=0.143)。当将分析限制为美托洛尔时,得到了相同的结果,但风险有所降低。
本研究发现,患有心脏病且使用高剂量β受体阻滞剂的孕妇发生 SGA 儿的风险增加了五倍,使用低剂量β受体阻滞剂的孕妇发生 SGA 儿的风险增加了两倍,提示存在明显的剂量-反应关系。因此,对于接受β受体阻滞剂治疗的心脏病孕妇,应密切监测胎儿生长情况。由于妊娠期间的药物治疗不仅与母亲有关,也与胎儿有关,因此应该达到母亲和胎儿的最佳平衡。