Khoshkar Yashar, Westerberg Marcus, Adolfsson Jan, Bill-Axelson Anna, Olsson Henrik, Eklund Martin, Akre Olof, Garmo Hans, Aly Markus
Department of Molecular Medicine and Surgery Karolinska Institute Stockholm Sweden.
Department of Mathematics Uppsala University Uppsala Sweden.
BJUI Compass. 2021 Oct 10;3(2):173-183. doi: 10.1002/bco2.116. eCollection 2022 Mar.
The objective of this study is to find clinical variables that predict the prognosis for men with castration-resistant prostate cancer (CRPC) in a Swedish real-life CRPC cohort, including a risk group classification to clarify the risk of succumbing to prostate cancer. This is a natural history cohort representing the premodern drug era before the introduction of novel hormonal drug therapies.
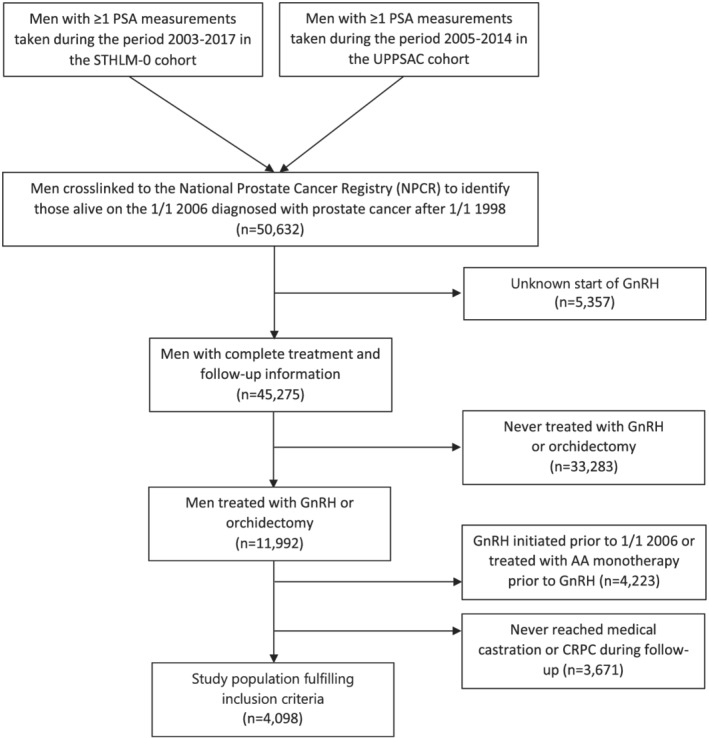
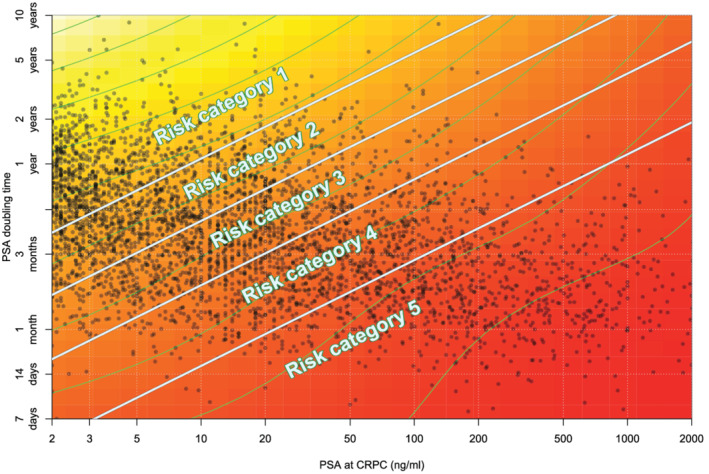
PSA tests from the clinical chemistry laboratories serving health care in six regions of Sweden were retrieved and cross-linked to the National Prostate Cancer Registry (NPCR) to identify men with a prostate cancer diagnosis. Through further cross-linking with data sources at the Swedish Board of Health and Welfare, we retrieved other relevant information such as prescribed drugs, hospitalizations, and cause of death. Men entered the CRPC cohort at the first date of doubling of their PSA nadir value with the last value being >2 ng/ml, or an absolute increase of >5 ng/ml or more, whilst on 3 months of medical castration or if they had been surgically castrated ( = 4098). By combining the two variables with the largest C-statistics, "PSA at time of CRPC" and "PSA doubling time," a risk group classification was created.
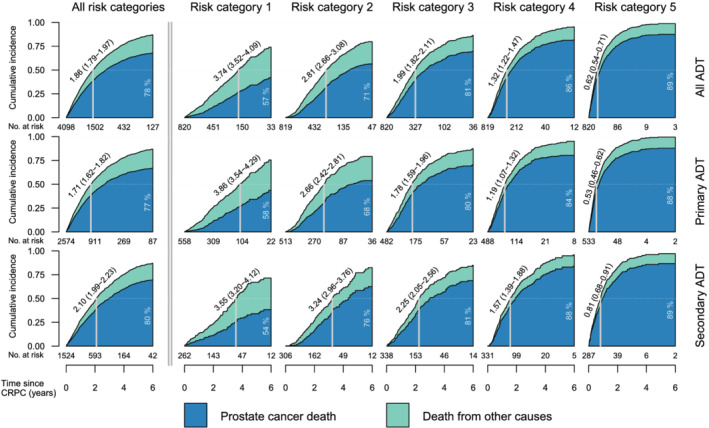
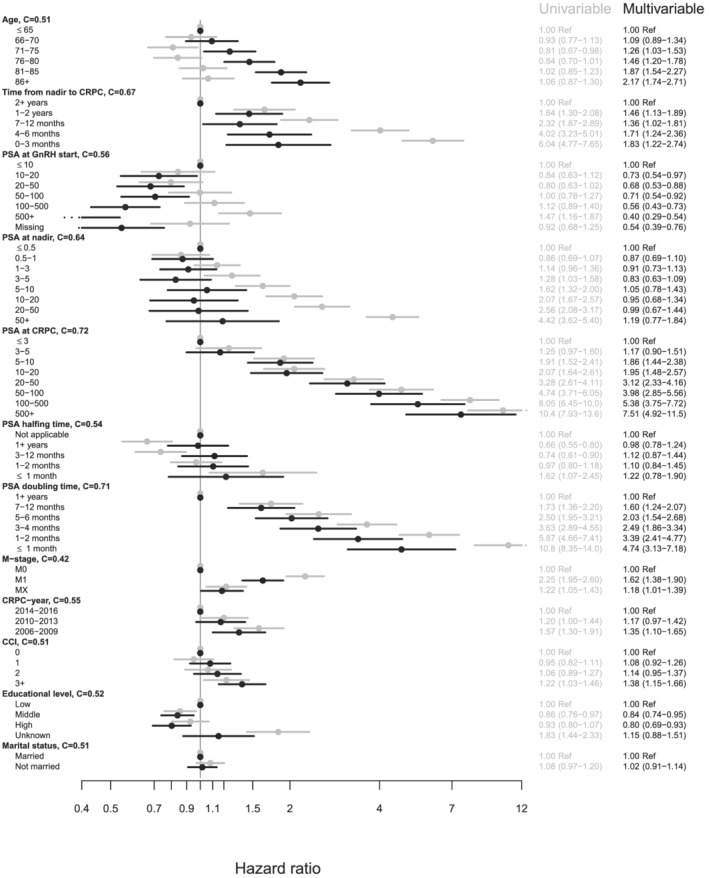
PSA-DT and PSA at date of CRPC are the strongest variables associated with PC specific survival. At the end of follow-up, the proportion of men who died due to PC was 57%, 71%, 81%, 86%, and 89% for risk categories one through five, respectively. The median overall survival in our cohort of men with CRPC was 1.86 years (95% CI: 1.79-1.97).
For a man with castration-resistant prostate cancer, there is a high probability that this will be the main cause contributing to his death. However, there is a significant difference in mortality that varies in relation to tumor burden assessed as PSA doubling time and PSA at time of CRCP. This information could be used in a clinical setting when deciding when to treat more or less aggressively once entering the CRPC phase of the disease.
本研究的目的是在瑞典真实世界的去势抵抗性前列腺癌(CRPC)队列中找出可预测男性患者预后的临床变量,包括进行风险分组以明确死于前列腺癌的风险。这是一个代表新型激素药物疗法引入之前的前现代药物时代的自然史队列。
检索了瑞典六个地区提供医疗保健服务的临床化学实验室的PSA检测结果,并将其与国家前列腺癌登记处(NPCR)进行交叉关联,以识别出前列腺癌确诊患者。通过与瑞典卫生和福利委员会的数据源进一步交叉关联,我们获取了其他相关信息,如处方药、住院情况和死亡原因。男性患者在其PSA最低点值翻倍且最后值>2 ng/ml的首日进入CRPC队列,或者在接受3个月药物去势治疗期间PSA绝对值增加>5 ng/ml或更多,或者接受过手术去势(n = 4098)。通过结合C统计量最大的两个变量“CRPC时的PSA”和“PSA翻倍时间”,创建了一个风险分组。
PSA翻倍时间(PSA-DT)和CRPC时的PSA是与前列腺癌特异性生存最相关的变量。随访结束时,一至五类风险组中因前列腺癌死亡的男性比例分别为57%、71%、81%、86%和89%。我们CRPC男性队列的中位总生存期为1.86年(95%置信区间:1.79 - 1.97)。
对于去势抵抗性前列腺癌男性患者,这很可能是导致其死亡的主要原因。然而,死亡率存在显著差异,其与根据PSA翻倍时间和CRPC时的PSA评估的肿瘤负荷相关。这些信息可在临床环境中用于决定疾病进入CRPC阶段后何时采取更积极或较保守的治疗。