Neuroimmunology Program, Institut d'Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain.
Neurology Service, Hospital Clinic de Barcelona, Barcelona, Spain.
Front Immunol. 2022 Apr 11;13:866153. doi: 10.3389/fimmu.2022.866153. eCollection 2022.
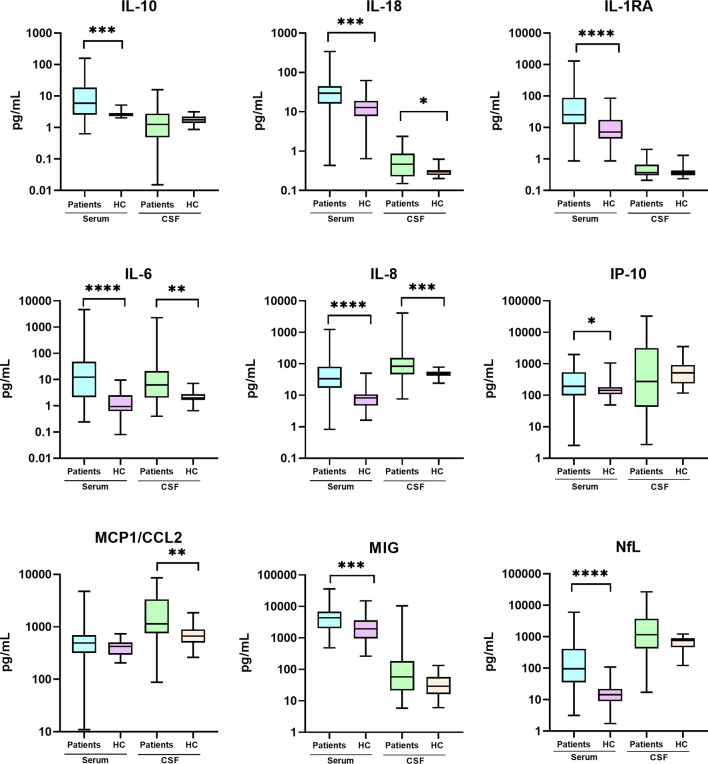
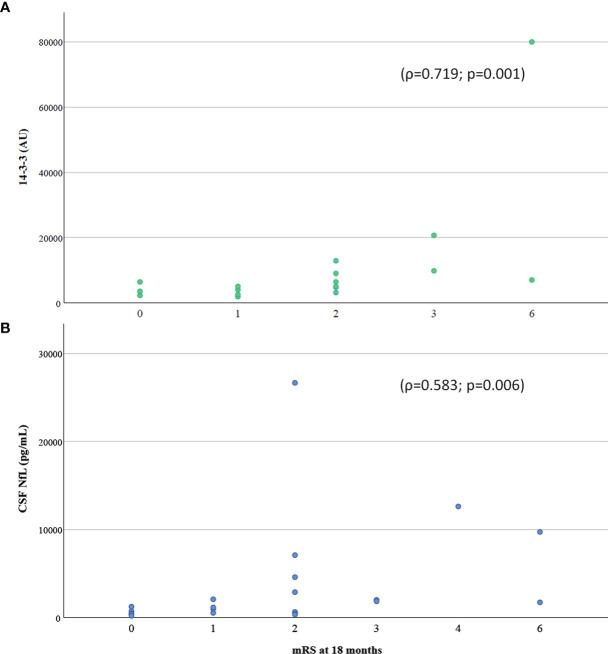
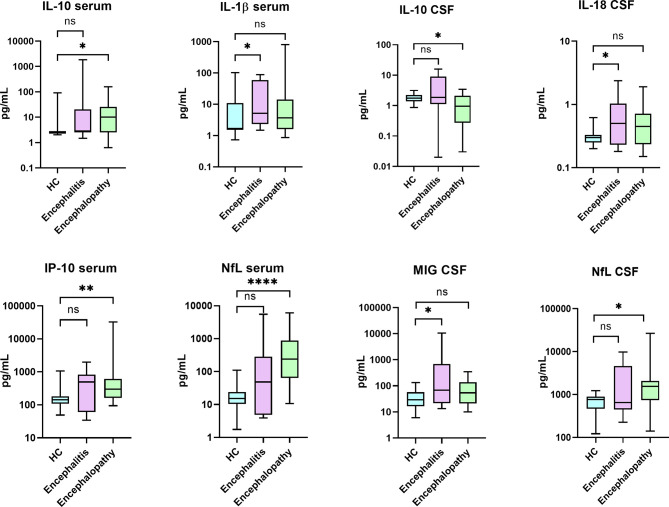
Patients with coronavirus disease 2019 (COVID-19) frequently develop acute encephalopathy and encephalitis, but whether these complications are the result from viral-induced cytokine storm syndrome or anti-neural autoimmunity is still unclear. In this study, we aimed to evaluate the diagnostic and prognostic role of CSF and serum biomarkers of inflammation (a wide array of cytokines, antibodies against neural antigens, and IgG oligoclonal bands), and neuroaxonal damage (14-3-3 protein and neurofilament light [NfL]) in patients with acute COVID-19 and associated neurologic manifestations (neuro-COVID). We prospectively included 60 hospitalized neuro-COVID patients, 25 (42%) of them with encephalopathy and 14 (23%) with encephalitis, and followed them for 18 months. We found that, compared to healthy controls (HC), neuro-COVID patients presented elevated levels of IL-18, IL-6, and IL-8 in both serum and CSF. MCP1 was elevated only in CSF, while IL-10, IL-1RA, IP-10, MIG and NfL were increased only in serum. Patients with COVID-associated encephalitis or encephalopathy had distinct serum and CSF cytokine profiles compared with HC, but no differences were found when both clinical groups were compared to each other. Antibodies against neural antigens were negative in both groups. While the levels of neuroaxonal damage markers, 14-3-3 and NfL, and the proinflammatory cytokines IL-18, IL-1RA and IL-8 significantly associated with acute COVID-19 severity, only the levels of 14-3-3 and NfL in CSF significantly correlated with the degree of neurologic disability in the daily activities at 18 months follow-up. Thus, the inflammatory process promoted by SARS-CoV-2 infection might include blood-brain barrier disruption in patients with neurological involvement. In conclusion, the fact that the levels of pro-inflammatory cytokines do not predict the long-term functional outcome suggests that the prognosis is more related to neuronal damage than to the acute neuroinflammatory process.
新型冠状病毒肺炎(COVID-19)患者常发生急性脑病和脑炎,但这些并发症是病毒诱导的细胞因子风暴综合征还是抗神经自身免疫的结果尚不清楚。在这项研究中,我们旨在评估脑脊液和血清炎症生物标志物(广泛的细胞因子、针对神经抗原的抗体和 IgG 寡克隆带)以及神经轴突损伤(14-3-3 蛋白和神经丝轻链[NfL])在急性 COVID-19 患者中的诊断和预后作用,并伴有神经 COVID-19 相关的神经系统表现。我们前瞻性纳入了 60 例住院的神经 COVID-19 患者,其中 25 例(42%)为脑病,14 例(23%)为脑炎,并对其进行了 18 个月的随访。我们发现,与健康对照组(HC)相比,神经 COVID-19 患者血清和脑脊液中 IL-18、IL-6 和 IL-8 的水平升高。MCP1 仅在脑脊液中升高,而 IL-10、IL-1RA、IP-10、MIG 和 NfL 仅在血清中升高。与 HC 相比,COVID 相关脑炎或脑病患者的血清和脑脊液细胞因子谱不同,但将两个临床组相互比较时,没有发现差异。两组患者的神经抗原抗体均为阴性。虽然神经轴突损伤标志物 14-3-3 和 NfL 以及促炎细胞因子 IL-18、IL-1RA 和 IL-8 的水平与急性 COVID-19 的严重程度显著相关,但只有脑脊液中 14-3-3 和 NfL 的水平与 18 个月随访时日常生活中的神经功能障碍程度显著相关。因此,SARS-CoV-2 感染引起的炎症过程可能包括神经受累患者的血脑屏障破坏。总之,促炎细胞因子的水平不能预测长期的功能预后,这表明预后与神经元损伤的关系更为密切,而与急性神经炎症过程的关系不密切。