Thomson Alistair, Totaro Richard, Cooper Wendy, Dennis Mark
Department of Intensive Care, Intensive Care Unit, Royal Prince Alfred Hospital, Sydney, Australia.
Department of Tissue Pathology and Diagnostic Oncology, NSW Health Pathology, Royal Prince Alfred Hospital, Sydney, Australia.
Eur Heart J Case Rep. 2022 Apr 13;6(4):ytac142. doi: 10.1093/ehjcr/ytac142. eCollection 2022 Apr.
Whilst myocarditis or myocardial injury due to severe acute respiratory syndrome coronavirus 2 infection is commonly reported, profound primary cardiac dysfunction requiring mechanical circulatory support, with the development of fulminant myocarditis prior to respiratory failure, is rarely described. The endomyocardial biopsy (EMB) findings in these patients is seldom reported, the findings are varied, and effective treatment unknown.
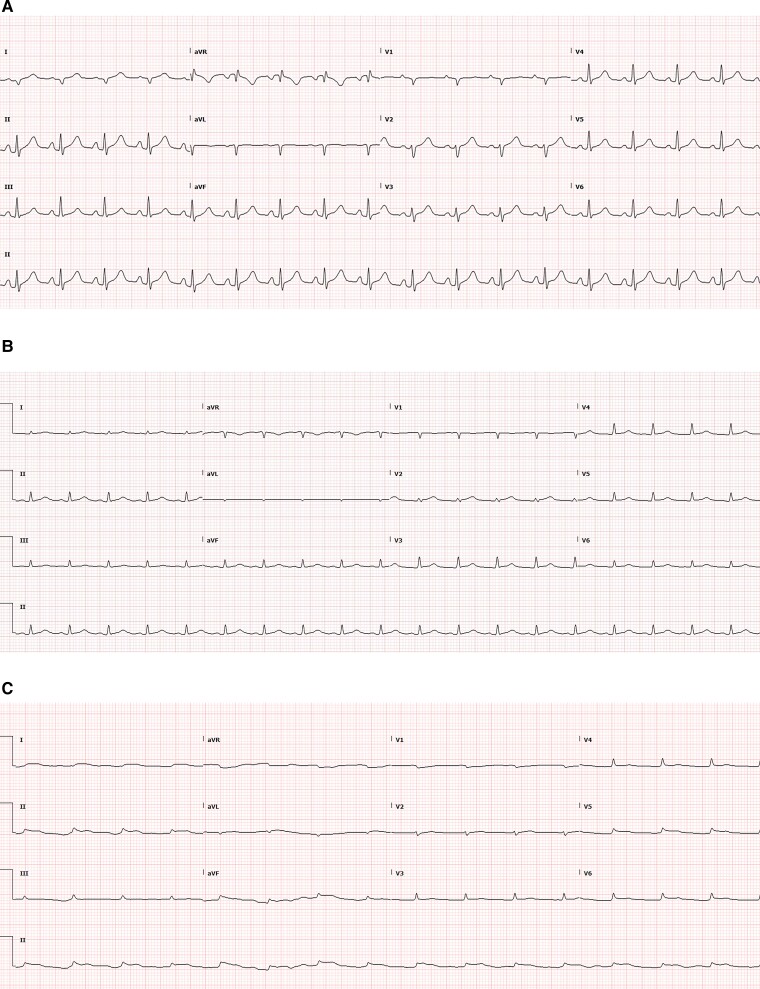
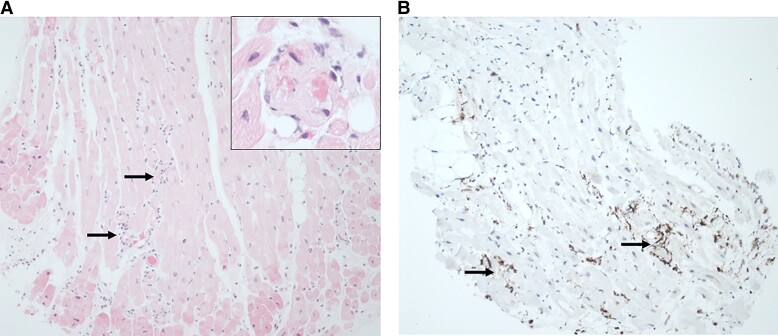
A 39-year-old female with no significant past medical history and confirmed Delta variant coronavirus disease 2019 (COVID-19) infection (Day 3), presented with a 1 day history of diarrhoea, vomiting, and abdominal pain. The patient denied respiratory symptoms and chest X-ray was clear. Lactate level was 6.3, initial troponin T 118 ng/L. Despite resuscitation, the patient significantly deteriorated in the emergency department, resulting in pulseless electrical activity arrest requiring veno-arterial extra-corporeal membrane oxygenation cardiopulmonary resuscitation. Over the following 36 h, cardiac function deteriorated to near-complete left ventricular (LV) standstill. Coronary angiography revealed normal coronary arteries with slow flow. Endomyocardial biopsy showed diffuse interstitial macrophage infiltrate and small vessel thromboses. Left ventricular function did not improve over the following 7 days, and despite treatment with tocilizumab, high-dose steroids, and intravenous immunoglobulin, she eventually died due to disease-related complications.
Primary cardiac dysfunction secondary to COVID-19 infection is rarely reported. Little is known about the incidence, natural history, and pathophysiology of fulminant COVID-19 myocarditis. We present the most severe case of cardiac dysfunction due to COVID-19 reported in a young patient without respiratory compromise who never recovered from any cardiac function.
虽然严重急性呼吸综合征冠状病毒2感染所致心肌炎或心肌损伤屡有报道,但在呼吸衰竭之前发展为暴发性心肌炎,需要机械循环支持的严重原发性心脏功能障碍却鲜有描述。这些患者的心内膜心肌活检(EMB)结果很少被报道,结果各异,且有效治疗方法不明。
一名39岁女性,既往无重大病史,确诊感染2019冠状病毒病(COVID-19)Delta变异株(第3天),出现腹泻、呕吐和腹痛1天。患者否认有呼吸道症状,胸部X光检查正常。乳酸水平为6.3,初始肌钙蛋白T为118 ng/L。尽管进行了复苏,但患者在急诊科病情显著恶化,导致无脉电活动骤停,需要进行静脉-动脉体外膜肺氧合心肺复苏。在接下来的36小时内,心脏功能恶化至近乎完全的左心室停搏。冠状动脉造影显示冠状动脉正常但血流缓慢。心内膜心肌活检显示弥漫性间质巨噬细胞浸润和小血管血栓形成。在接下来的7天里,左心室功能没有改善,尽管使用了托珠单抗、大剂量类固醇和静脉注射免疫球蛋白治疗,但她最终因疾病相关并发症死亡。
COVID-19感染继发的原发性心脏功能障碍鲜有报道。对于暴发性COVID-19心肌炎的发病率、自然史和病理生理学知之甚少。我们报告了一名年轻患者中因COVID-19导致的最严重心脏功能障碍病例,该患者无呼吸功能损害,心脏功能从未恢复。