Nursing Department, Quality of care, University Hospitals of Geneva, Geneva, Switzerland
Quality of Care Service, University Hospitals of Geneva, Geneva, Switzerland.
BMJ Open Qual. 2022 Apr;11(2). doi: 10.1136/bmjoq-2021-001699.
Infection prevention and control (IPC) is a prioritised task for healthcare workers in emergency department (ED). Here, we examined compliance with admission screening (AS) and additional precautions (AP) measures for patients at risk of infection with multidrug-resistant organisms (MDROs) by using a two-stage, multifaceted educational intervention, also comparing the cost of a developed automated indicator for AS and AP compliance and clinical audits to sustain observed findings.
In the first stage, staff in the ED of the University Hospitals of Geneva, Switzerland, were briefed on IPC measures (AS and AP). A cross-sectional survey was then conducted to assess barriers to IPC measures. In the second stage, healthcare workers underwent training sessions, and an electronic patient record 'order-set' including AS and AP compliance indicators was designed. We compared the cost-benefit of the audits and the automated indicators for AS and AP compliance.
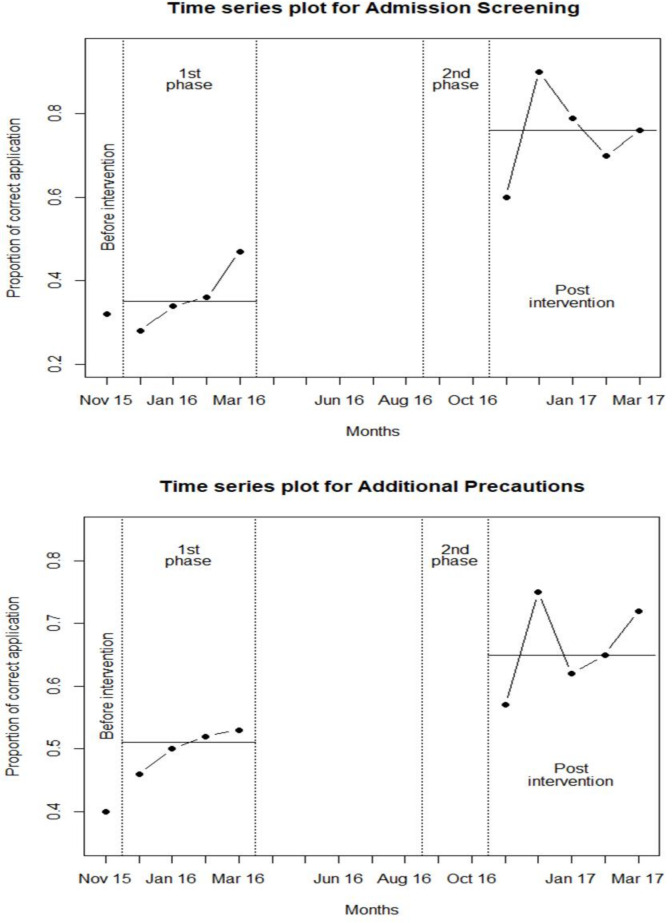
Compliance significantly improved after training, from 36.2% (95% CI 23.6% to 48.8%) to 78.8% (95% CI 67.1% to 90.3%) for AS (n=100, p=0.0050) and from 50.2% (95% CI 45.3% to 55.1%) to 68.5% (95% CI 60.1% to 76.9%) for AP (n=125, p=0.0092). Healthcare workers recognised MDRO screening as an ED task (70.2%), with greater acknowledgment of risk factors at AS considered an ED duty. The monthly cost was higher for clinical audits than the automated indicator, with a reported yearly cost of US$120 203. The initial cost of developing the automated indicator was US$18 290 and its return on investment US$3.44 per US$1 invested.
Training ED staff increased compliance with IPC measures when accompanied by team discussions for optimal effectiveness. An automated indicator of compliance is cheaper and closer to real-time than a clinical audit.
感染预防与控制(IPC)是急诊科医护人员的首要任务。在这里,我们通过两阶段、多方面的教育干预措施,检查了对感染多重耐药菌(MDRO)风险患者的入院筛查(AS)和附加预防措施(AP)措施的依从性,并比较了为 AS 和 AP 依从性和临床审计开发的自动化指标的成本,以维持观察到的结果。
在第一阶段,瑞士日内瓦大学医院的急诊科工作人员接受了 IPC 措施(AS 和 AP)的培训。然后进行了横断面调查,以评估 IPC 措施的障碍。在第二阶段,医护人员接受了培训课程,并设计了一个包含 AS 和 AP 依从性指标的电子病历“医嘱集”。我们比较了审计和自动化指标在 AS 和 AP 依从性方面的成本效益。
培训后,AS 的依从性从 36.2%(95%CI 23.6%至 48.8%)显著提高到 78.8%(95%CI 67.1%至 90.3%)(n=100,p=0.0050),AP 的依从性从 50.2%(95%CI 45.3%至 55.1%)显著提高到 68.5%(95%CI 60.1%至 76.9%)(n=125,p=0.0092)。医护人员将 MDRO 筛查视为急诊科任务(70.2%),并认为在 AS 时更应认识到危险因素。与自动化指标相比,临床审计的每月成本更高,报告的年成本为 120203 美元。开发自动化指标的初始成本为 18290 美元,投资回报率为每投资 1 美元 3.44 美元。
培训急诊科工作人员并辅以团队讨论以提高 IPC 措施的依从性,可实现最佳效果。与临床审计相比,依从性的自动化指标更便宜且更接近实时。