Institute for Systems Biology, 401 Terry Ave N, Seattle, WA, 98109, USA.
Washington University School of Medicine, St. Louis, MO, 63110, USA.
Sci Rep. 2022 Apr 28;12(1):6568. doi: 10.1038/s41598-022-10344-3.
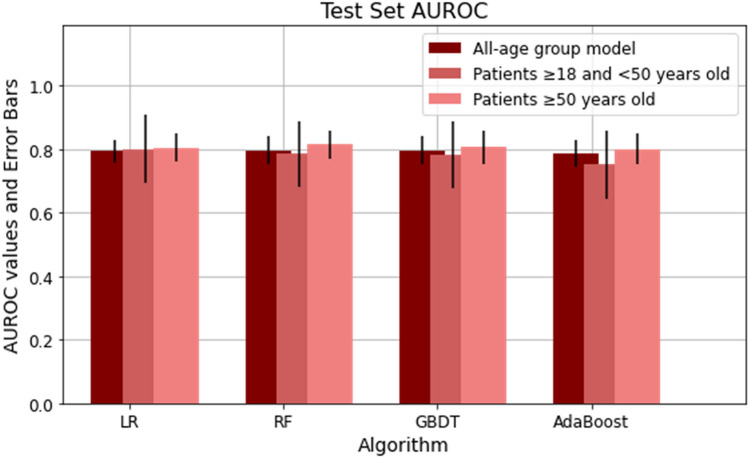
Risk stratification for hospitalized adults with COVID-19 is essential to inform decisions about individual patients and allocation of resources. So far, risk models for severe COVID outcomes have included age but have not been optimized to best serve the needs of either older or younger adults. Models also need to be updated to reflect improvements in COVID-19 treatments. This retrospective study analyzed data from 6906 hospitalized adults with COVID-19 from a community health system across five states in the western United States. Risk models were developed to predict mechanical ventilation illness or death across one to 56 days of hospitalization, using clinical data available within the first hour after either admission with COVID-19 or a first positive SARS-CoV-2 test. For the seven-day interval, models for age ≥ 18 and < 50 years reached AUROC 0.81 (95% CI 0.71-0.91) and models for age ≥ 50 years reached AUROC 0.82 (95% CI 0.77-0.86). Models revealed differences in the statistical significance and relative predictive value of risk factors between older and younger patients including age, BMI, vital signs, and laboratory results. In addition, for hospitalized patients, sex and chronic comorbidities had lower predictive value than vital signs and laboratory results.
对住院的 COVID-19 成年患者进行风险分层对于告知患者个体和资源分配决策至关重要。到目前为止,严重 COVID 结局的风险模型包括年龄,但尚未经过优化以最好地满足老年或年轻成年人的需求。模型还需要更新,以反映 COVID-19 治疗方法的改进。本回顾性研究分析了来自美国西部五个州一个社区卫生系统的 6906 名住院 COVID-19 成年患者的数据。使用 COVID-19 入院或首次 SARS-CoV-2 检测呈阳性后第一小时内可用的临床数据,开发了预测机械通气疾病或住院后 1 至 56 天内死亡的风险模型。对于 7 天的间隔,年龄≥18 岁且<50 岁的模型的 AUROC 为 0.81(95%CI 0.71-0.91),年龄≥50 岁的模型的 AUROC 为 0.82(95%CI 0.77-0.86)。模型揭示了年龄、BMI、生命体征和实验室结果等危险因素在老年和年轻患者之间的统计学意义和相对预测价值的差异。此外,对于住院患者,性别和慢性合并症的预测价值低于生命体征和实验室结果。