School of Basic Medicine, Guangzhou University of Chinese Medicine, Guangzhou, 510006, Guangdong Province, China.
Zhongshan Hospital of Chinese Medicine, No. 3 Kangxin Road, Xi District, Zhongshan, 528400, Guangdong Province, China.
Sci Rep. 2022 Apr 28;12(1):6977. doi: 10.1038/s41598-022-10996-1.
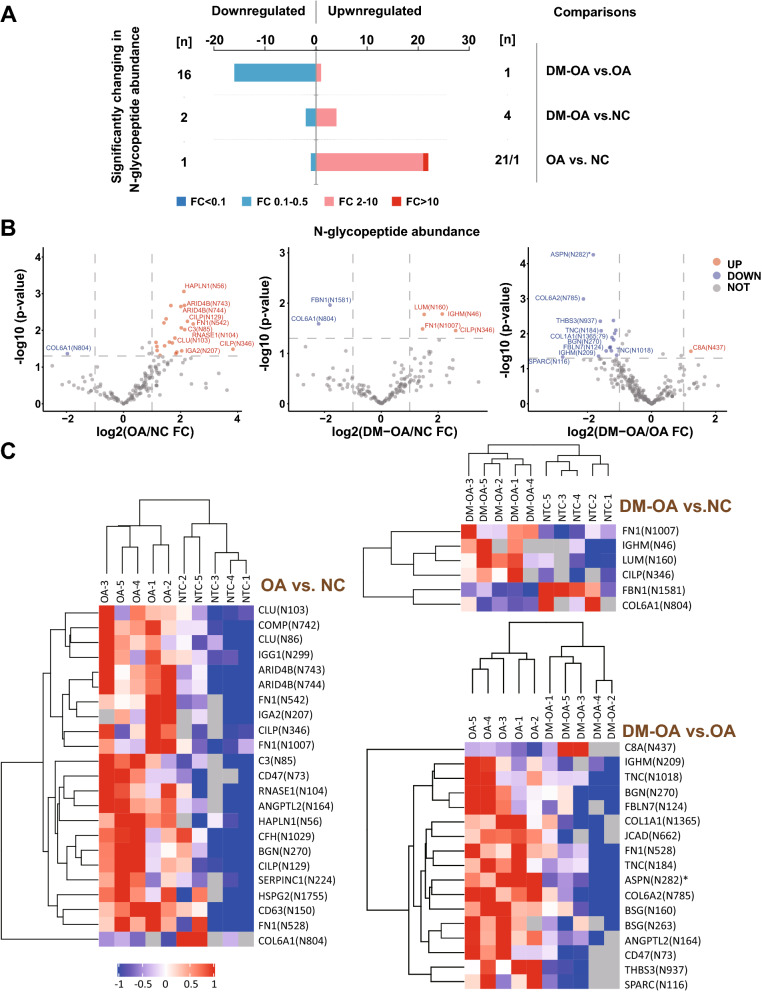
Whether the relationship between type 2 diabetes mellitus (T2DM) and osteoarthritis (OA) can be solely attributed to the shared risk factors, such as obesity, remains controversial. Several studies have revealed the critical role of abnormal glycosylation in the pathogenesis of OA and T2DM. Therefore, we speculate that T2DM may contribute to the pathogenesis of OA through the intrinsic mechanisms of N-glycosylation aberrations. Using N-glycoproteomics, we compared the changes in N-glycosylated protein abundance in cartilage samples from patients with OA without and with T2DM (DM-OA), and from patients with traumatic joint injury (NC) as controls. We identified 847 N-glycosylation sites corresponding to 729 peptides fragments from 374 proteins. The number of N-glycosylated proteins in the DM-OA group tended to decrease compared with that in the OA and NC groups. We identified 22 upregulated and 1 down-regulated N-glycosylated peptides in the OA group compared to the NC group, while only fibronectin 1 (FN1) at position N1007, cartilage intermediate layer protein 1 (CILP) at N346, and collagen type VI alpha 1 chain (COL6A1) at N804, were also identified in the DM-OA group. Compared to the OA group, the downregulation of secreted protein acidic and rich in cysteine (SPARC) at N116, collagen type VI alpha 1 chain (COL6A2) at N785, and asporin (ASPN) at N282, and the upregulation of complement component C8 alpha chain (C8α) at N437, were the most remarkable alterations in the DM-OA group. The differentially expressed N-glycosylated proteins between the OA and DM-OA groups were mainly located extracellularly and enriched in the KEGG pathways involving PI3K/Akt signaling, focal adhesion, and ECM-receptor interaction. Their predicted protein-protein interactions were also depicted. We were thus able to show the general characteristics of N-glycosylation aberrations in OA and DM-OA. Moreover, the upregulated glycosylated complement C8α in the DM-OA group might augment membrane attack complex activity, thereby exacerbating cartilage destruction. Although further confirmation is required, our hypothesis proposes a possible explanation for the deduction that T2DM is an independent risk factor for OA.
2 型糖尿病(T2DM)与骨关节炎(OA)之间的关系是否仅归因于肥胖等共同的危险因素,仍存在争议。几项研究揭示了异常糖基化在 OA 和 T2DM 发病机制中的关键作用。因此,我们推测 T2DM 可能通过 N-糖基化异常的内在机制导致 OA 的发病。我们使用 N-糖蛋白质组学比较了 OA 患者(DM-OA)和创伤性关节损伤患者(NC)软骨样本中 N-糖基化蛋白丰度的变化,以作为对照组。我们从 374 种蛋白质中鉴定出 729 个肽片段对应的 847 个 N-糖基化位点。与 OA 和 NC 组相比,DM-OA 组的 N-糖基化蛋白数量趋于减少。与 NC 组相比,OA 组中鉴定出 22 个上调和 1 个下调的 N-糖基化肽,而在 DM-OA 组中还鉴定出纤维连接蛋白 1(FN1)在 N1007 位、软骨中间层蛋白 1(CILP)在 N346 位和胶原 VI ɑ1 链(COL6A1)在 N804 位。与 OA 组相比,DM-OA 组中分泌型酸性富含半胱氨酸蛋白(SPARC)在 N116 位、胶原 VI ɑ1 链(COL6A2)在 N785 位和天冬氨酸蛋白酶抑制剂(ASPN)在 N282 位的下调,以及补体成分 C8α 链(C8α)在 N437 位的上调最为显著。OA 和 DM-OA 组之间差异表达的 N-糖基化蛋白主要位于细胞外,富集在涉及 PI3K/Akt 信号通路、焦点黏附和 ECM-受体相互作用的 KEGG 途径中。还描绘了它们预测的蛋白质-蛋白质相互作用。因此,我们能够展示 OA 和 DM-OA 中 N-糖基化异常的一般特征。此外,DM-OA 组中上调的糖基化补体 C8α 可能增强膜攻击复合物的活性,从而加剧软骨破坏。尽管需要进一步确认,但我们的假设提出了一个可能的解释,即 T2DM 是 OA 的一个独立危险因素。