LSE Health, London School of Economics and Political Science, London, UK
School of Human Sciences, University of Greenwich, Greenwich, London, UK.
BMJ Glob Health. 2022 Apr;7(4). doi: 10.1136/bmjgh-2022-008604.
Prompt access to emergency obstetrical care (EmOC) reduces the risk of maternal mortality. We assessed institutional maternal mortality by distance and travel time for pregnant women with obstetrical emergencies in Lagos State, Nigeria.
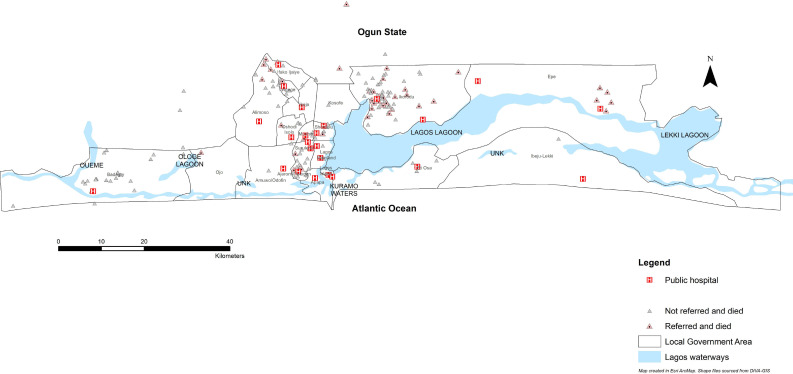
We conducted a facility-based retrospective cohort study across 24 public hospitals in Lagos. Reviewing case notes of the pregnant women presenting between 1 November 2018 and 30 October 2019, we extracted socio-demographic, travel and obstetrical data. The extracted travel data were exported to Google Maps, where driving distance and travel time data were extracted. Multivariable logistic regression was conducted to determine the relative influence of distance and travel time on maternal death.
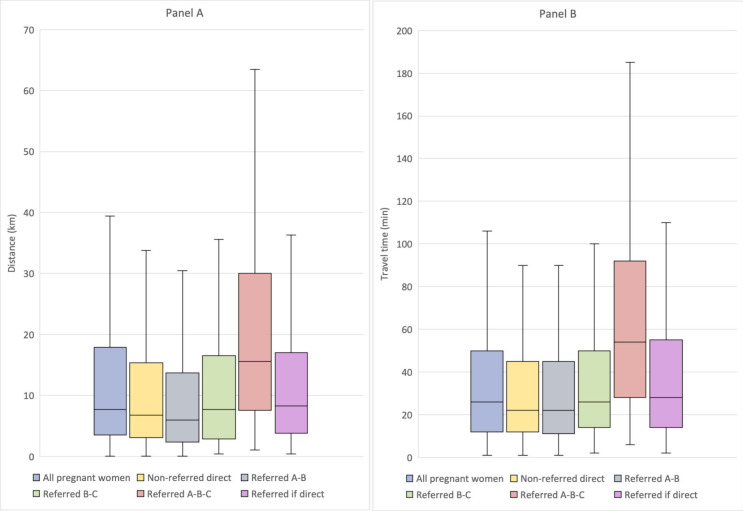
Of 4181 pregnant women with obstetrical emergencies, 182 (4.4%) resulted in maternal deaths. Among those who died, 60.3% travelled ≤10 km directly from home, and 61.9% arrived at the hospital ≤30 mins. The median distance and travel time to EmOC was 7.6 km (IQR 3.4-18.0) and 26 mins (IQR 12-50). For all women, travelling 10-15 km (2.53, 95% CI 1.27 to 5.03) was significantly associated with maternal death. Stratified by referral, odds remained statistically significant for those travelling 10-15 km in the non-referred group (2.48, 95% CI 1.18 to 5.23) and for travel ≥120 min (7.05, 95% CI 1.10 to 45.32). For those referred, odds became statistically significant at 25-35 km (21.40, 95% CI 1.24 to 36.72) and for journeys requiring travel time from as little as 10-29 min (184.23, 95% CI 5.14 to 608.51). Odds were also significantly higher for women travelling to hospitals in suburban (3.60, 95% CI 1.59 to 8.18) or rural (2.51, 95% CI 1.01 to 6.29) areas.
Our evidence shows that distance and travel time influence maternal mortality differently for referred women and those who are not. Larger scale research that uses closer-to-reality travel time and distance estimates as we have done, rethinking of global guidelines, and bold actions addressing access gaps, including within the suburbs, will be critical in reducing maternal mortality by 2030.
及时获得紧急产科护理(EmOC)可降低产妇死亡率。我们评估了尼日利亚拉各斯州因产科急症接受治疗的孕妇的机构产妇死亡率与距离和出行时间的关系。
我们对拉各斯的 24 家公立医院进行了基于机构的回顾性队列研究。对 2018 年 11 月 1 日至 2019 年 10 月 30 日期间就诊的孕妇的病历进行了回顾,提取了社会人口统计学、旅行和产科数据。提取的旅行数据被导出到谷歌地图,从中提取了驾车距离和旅行时间数据。采用多变量逻辑回归来确定距离和旅行时间对产妇死亡的相对影响。
在 4181 名患有产科急症的孕妇中,有 182 名(4.4%)导致产妇死亡。在死亡的孕妇中,60.3%直接从家中出发的距离≤10 公里,61.9%到达医院的时间≤30 分钟。EmOC 的中位数距离和旅行时间分别为 7.6 公里(IQR 3.4-18.0)和 26 分钟(IQR 12-50)。对于所有女性,旅行 10-15 公里(2.53,95%CI 1.27 至 5.03)与产妇死亡显著相关。按转诊情况分层,在未转诊组中,旅行 10-15 公里的女性的比值仍然具有统计学意义(2.48,95%CI 1.18 至 5.23),旅行时间≥120 分钟的比值也具有统计学意义(7.05,95%CI 1.10 至 45.32)。对于转诊的孕妇,旅行距离为 25-35 公里(21.40,95%CI 1.24 至 36.72)和旅行时间为 10-29 分钟(184.23,95%CI 5.14 至 608.51)时,比值变得具有统计学意义。对于前往郊区(3.60,95%CI 1.59 至 8.18)或农村(2.51,95%CI 1.01 至 6.29)地区医院的女性,比值也显著升高。
我们的证据表明,距离和旅行时间对转诊女性和非转诊女性的产妇死亡率有不同的影响。更大规模的研究使用我们所做的更接近现实的旅行时间和距离估计,重新思考全球指南,并采取大胆行动解决获取服务的差距,包括在郊区,将对 2030 年降低产妇死亡率至关重要。