Institute of Metabolism and Systems Research, College of Medical and Dental Sciences, University of Birmingham, Birmingham, UK.
Centre for Endocrinology, Diabetes and Metabolism, Birmingham Health Partners, Birmingham, UK.
J Neuroendocrinol. 2022 Aug;34(8):e13118. doi: 10.1111/jne.13118. Epub 2022 May 1.
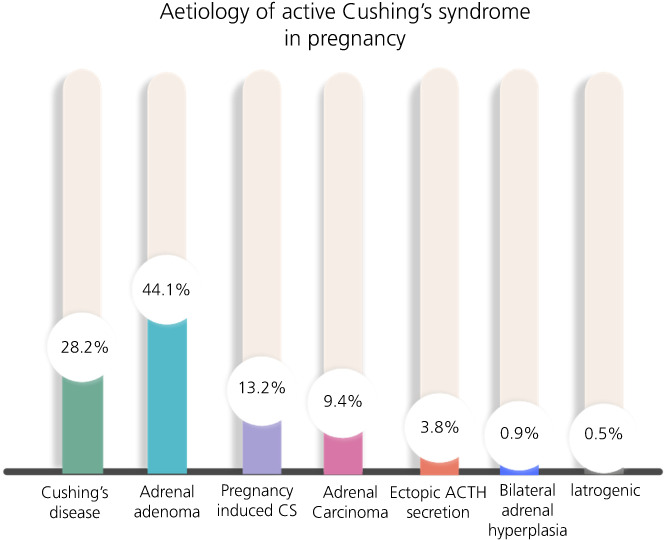
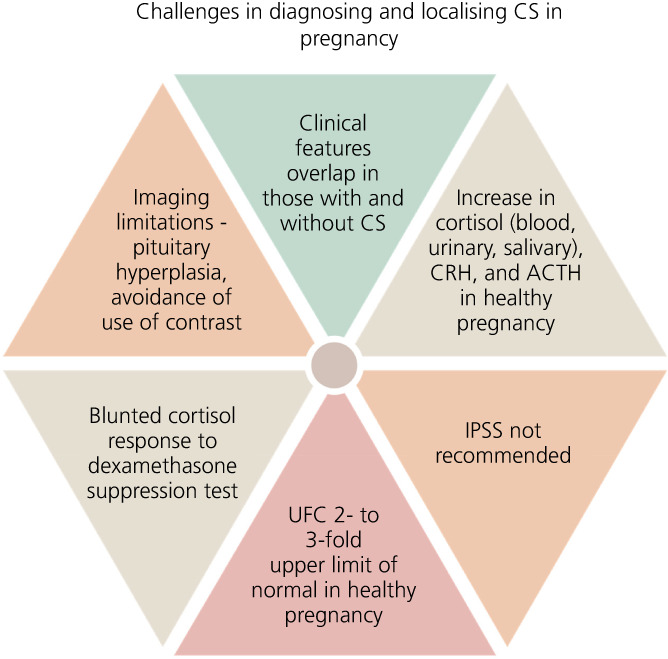
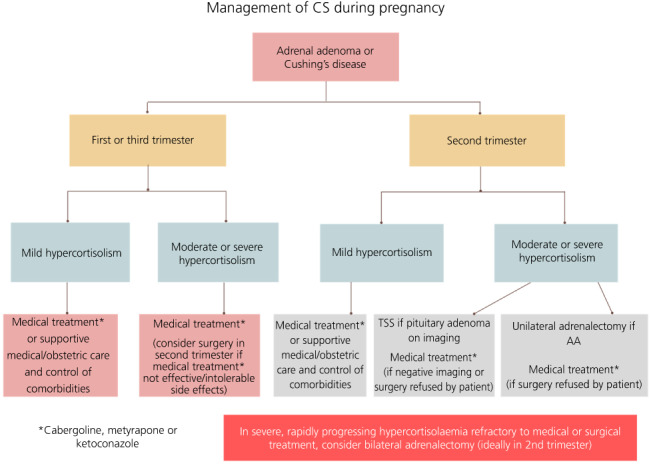
Endogenous Cushing's syndrome (CS) is rarely encountered during pregnancy. Clinical and biochemical changes in healthy pregnancy overlap with those seen in pregnancy complicated by CS; the diagnosis is therefore challenging and can be delayed. During normal gestation, adrenocorticotrophic hormone, corticotrophin-releasing hormone, cortisol, and urinary free cortisol levels rise. Dexamethasone administration fails to fully suppress cortisol in pregnant women without CS. Localisation may be hindered by non-suppressed adrenocorticotrophic hormone levels in a large proportion of those with adrenal CS; smaller corticotroph adenomas may go undetected as a result of a lack of contrast administration or the presence of pituitary hyperplasia; and inferior petrosal sinus sampling is not recommended given the risk of radiation and thrombosis. Yet, diagnosis is essential; active disease is associated with multiple insults to both maternal and foetal health, and those cured may normalise the risk of maternal-foetal complications. The published literature consists mostly of case reports or small case series affected by publication bias, heterogeneous definitions of maternal or foetal outcomes or lack of detail on severity of hypercortisolism. Consequently, conclusive recommendations, or a standardised management approach for all, cannot be made. Management is highly individualised: the decision for surgery, medical control of hypercortisolism or adoption of a conservative approach is dependent on the timing of diagnosis (respective to stage of gestation), the ability to localise the tumour, severity of CS, pre-existing maternal comorbidity, and, ultimately, patient choice. Close communication is a necessity with the patient placed at the centre of all decisions, with risks, benefits, and uncertainties around any investigation and management carefully discussed. Care should be delivered by an experienced, multidisciplinary team, with the resources and expertise available to manage such a rare and challenging condition during pregnancy.
内源性库欣综合征(CS)在怀孕期间很少见。健康妊娠的临床和生化变化与 CS 合并妊娠时所见重叠;因此,诊断具有挑战性且可能会延迟。在正常妊娠期间,促肾上腺皮质激素、促肾上腺皮质激素释放激素、皮质醇和尿游离皮质醇水平升高。在没有 CS 的孕妇中,地塞米松给药不能完全抑制皮质醇。在很大一部分肾上腺 CS 患者中,由于促肾上腺皮质激素水平未被抑制,定位可能会受到阻碍;由于缺乏对比剂给药或存在垂体增生,较小的促肾上腺皮质瘤可能无法被发现;并且由于存在辐射和血栓形成的风险,不建议进行蝶窦采样。然而,诊断至关重要;活动性疾病与母婴健康的多重损害有关,治愈的患者可能会使母婴并发症的风险正常化。已发表的文献主要由病例报告或小病例系列组成,受到发表偏倚、母体或胎儿结局的定义不同或缺乏对皮质醇增多症严重程度的详细信息的影响。因此,无法做出明确的结论性建议或为所有人制定标准化的管理方法。管理是高度个体化的:手术、皮质醇过度分泌的药物控制或保守方法的决策取决于诊断的时间(与妊娠阶段相对应)、肿瘤定位的能力、CS 的严重程度、母体预先存在的合并症,以及最终取决于患者的选择。与患者进行密切沟通,将患者置于所有决策的中心,仔细讨论任何检查和管理的风险、益处和不确定性。应通过有经验的多学科团队提供护理,该团队具备在怀孕期间管理这种罕见和具有挑战性的疾病的资源和专业知识。