Sharma Divyansh, Spring Kevin J, Bhaskar Sonu M M
Global Health Neurology and Translational Neuroscience Laboratory, Sydney and Neurovascular Imaging Laboratory, Clinical Sciences Stream, Ingham Institute for Applied Medical Research, Sydney, NSW, Australia.
South-Western Sydney Clinical School, University of New South Wales (UNSW), Sydney, NSW, Australia.
J Cent Nerv Syst Dis. 2022 Apr 22;14:11795735221092518. doi: 10.1177/11795735221092518. eCollection 2022.
Inflammation may mediate response to acute reperfusion therapy (RT) in acute cerebral ischaemia. Neutrophil-lymphocyte ratio (NLR), an inflammatory biomarker, may play an important role in acute ischaemic stroke (AIS) prognostication.
This meta-analysis sought to examine the effect of NLR on functional outcomes, mortality and adverse outcomes in AIS patients receiving RT.
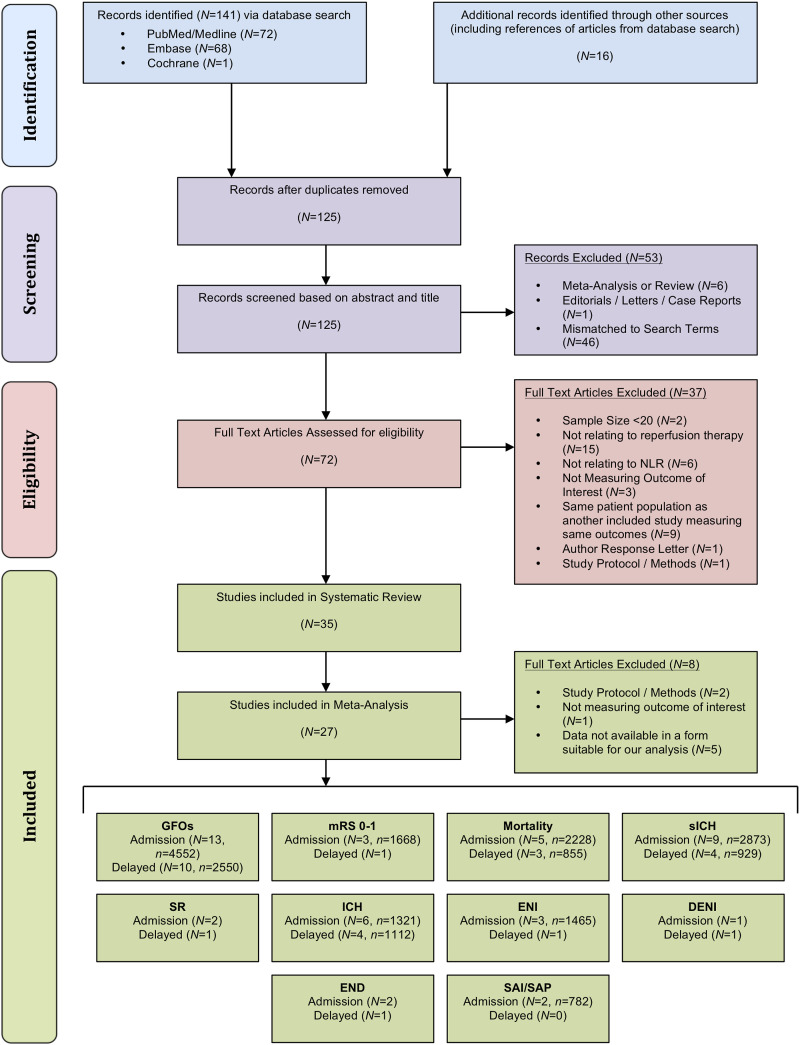
Individual studies were retrieved from PubMed/Medline, EMBASE and Cochrane databases. Data were extracted using a standardised data sheet and meta-analysis on association of admission (pre-RT) or delayed (post-RT) NLR with clinical/safety outcomes after RT was conducted.
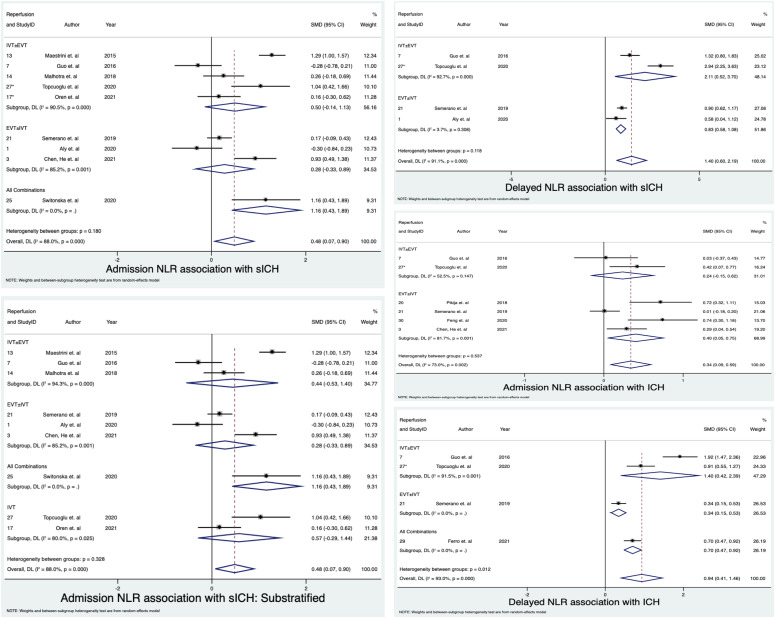
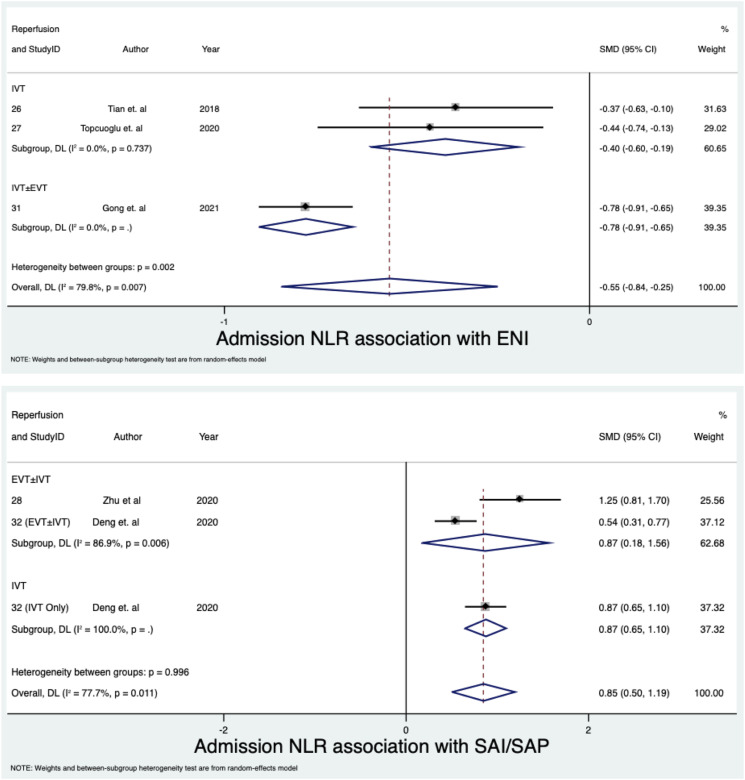
Thirty-five studies (n = 10 308) were identified for the systematic review with 27 (n = 8537) included in the meta-analyses. Lower admission NLR was associated with good functional outcomes (GFOs), defined as 3-month modified Rankin scale (mRS) 0-2 (SMD = -.46; 95% CI = -.62 to -.29; P < .0001), mRS 0-1 (SMD = -.44; 95% CI = -.66 to -.22; P < .0001) and early neurological improvement (ENI) (SMD = -.55; 95 %CI = -.84 to -.25; P < .0001). Lower delayed admission NLR was also associated with GFOs (SMD = -.80; 95%CI = -.91 to -.68; P < .0001). Higher admission NLR was significantly associated with mortality (SMD = .49; 95%CI = .12 to .85; P = .009), intracerebral haemorrhage (ICH) (SMD = .34; 95% CI = .09 to .59; P = .007), symptomatic ICH (sICH) (SMD = .48; 95% CI = .07 to .90; P = .022) and stroke-associated infection or pneumonia (SMD = .85; 95% CI = .50, 1.19; P < .0001). Higher delayed NLR was significantly associated with sICH (SMD = 1.40; 95% CI = .60 to 2.19; P = .001), ICH (SMD = .94; 95% CI = .41 to 1.46; P < .0001) and mortality (SMD = 1.12; 95% CI = .57 to 1.67; P < .0001). There were variations in outcomes across RT groups.
Higher admission or delayed NLR is significantly associated with worse morbidity, mortality and safety outcomes in AIS patients receiving RT.
炎症可能介导急性脑缺血时对急性再灌注治疗(RT)的反应。中性粒细胞与淋巴细胞比值(NLR)作为一种炎症生物标志物,可能在急性缺血性卒中(AIS)的预后中发挥重要作用。
本荟萃分析旨在研究NLR对接受RT的AIS患者功能结局、死亡率和不良结局的影响。
从PubMed/Medline、EMBASE和Cochrane数据库中检索个体研究。使用标准化数据表提取数据,并对RT后入院时(RT前)或延迟时(RT后)NLR与临床/安全结局的相关性进行荟萃分析。
共识别出35项研究(n = 10308)用于系统评价,其中27项(n = 8537)纳入荟萃分析。较低的入院时NLR与良好的功能结局(GFOs)相关,定义为3个月改良Rankin量表(mRS)评分为0 - 2(标准化均数差[SMD] = -0.46;95%置信区间[CI] = -0.62至 -0.29;P < 0.0001)、mRS评分为0 - 1(SMD = -0.44;95% CI = -0.66至 -0.22;P < 0.0001)以及早期神经功能改善(ENI)(SMD = -0.55;95% CI = -0.84至 -0.25;P < 0.0001)。较低的延迟入院时NLR也与GFOs相关(SMD = -0.80;95% CI = -0.91至 -0.68;P < 0.0001)。较高的入院时NLR与死亡率(SMD = 0.49;95% CI = 0.12至0.85;P = 0.009)、脑出血(ICH)(SMD = 0.34;95% CI = 0.09至0.59;P = 0.007)、症状性ICH(sICH)(SMD = 0.48;95% CI = 0.07至0.90;P = 0.022)以及卒中相关感染或肺炎(SMD = 0.85;95% CI = 0.50, 1.19;P < 0.0001)显著相关。较高的延迟NLR与sICH(SMD = 1.40;95% CI = 0.60至2.19;P = 0.001)、ICH(SMD = 0.94;95% CI = 0.41至1.46;P < 0.0001)和死亡率(SMD = 1.12;95% CI = 0.57至1.67;P < 0.0001)显著相关。不同RT组的结局存在差异。
较高的入院时或延迟时NLR与接受RT的AIS患者更差的发病率、死亡率和安全结局显著相关。