Beaudreault Cameron P, Muh Carrie R, Naftchi Alexandria, Spirollari Eris, Das Ankita, Vazquez Sima, Sukul Vishad V, Overby Philip J, Tobias Michael E, McGoldrick Patricia E, Wolf Steven M
New York Medical College, Valhalla, NY, United States.
Department of Neurosurgery, Westchester Medical Center, Valhalla, NY, United States.
Front Hum Neurosci. 2022 Apr 12;16:876204. doi: 10.3389/fnhum.2022.876204. eCollection 2022.
Responsive neurostimulation (RNS System) has been utilized as a treatment for intractable epilepsy. The RNS System delivers stimulation in response to detected abnormal activity, via leads covering the seizure foci, in response to detections of predefined epileptiform activity with the goal of decreasing seizure frequency and severity. While thalamic leads are often implanted in combination with cortical strip leads, implantation and stimulation with bilateral thalamic leads alone is less common, and the ability to detect electrographic seizures using RNS System thalamic leads is uncertain.
The present study retrospectively evaluated fourteen patients with RNS System depth leads implanted in the thalamus, with or without concomitant implantation of cortical strip leads, to determine the ability to detect electrographic seizures in the thalamus. Detailed patient presentations and lead trajectories were reviewed alongside electroencephalographic (ECoG) analyses.
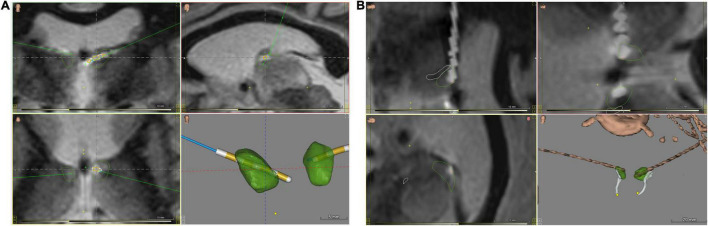
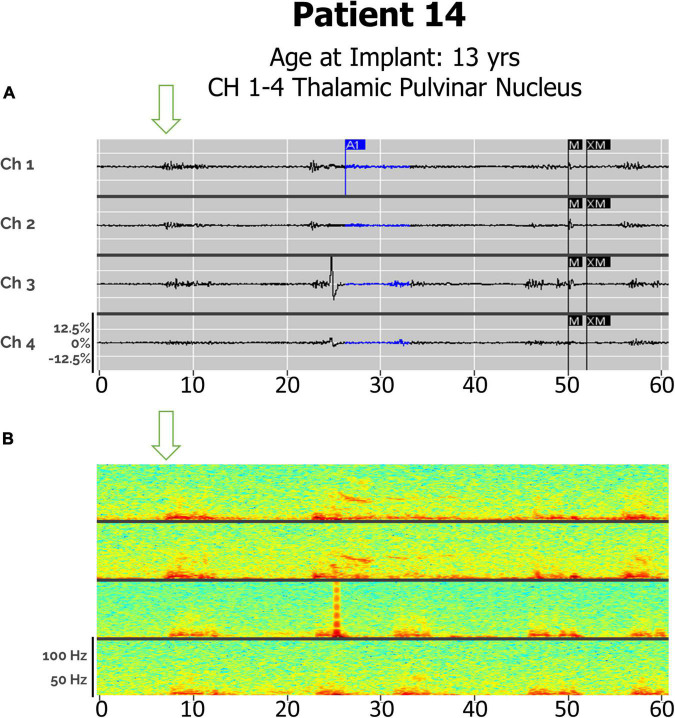
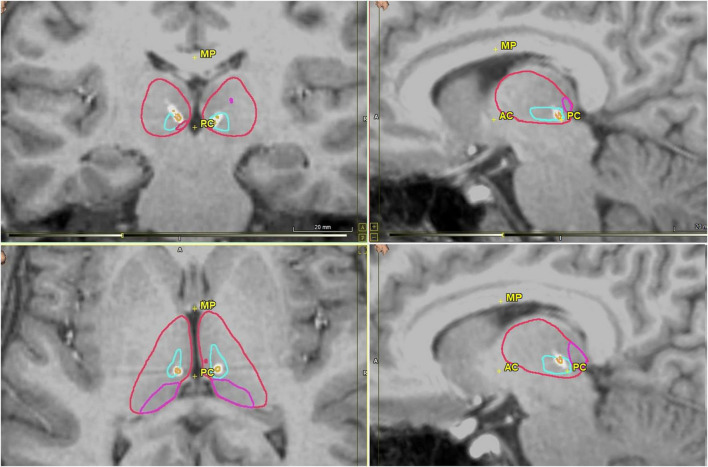
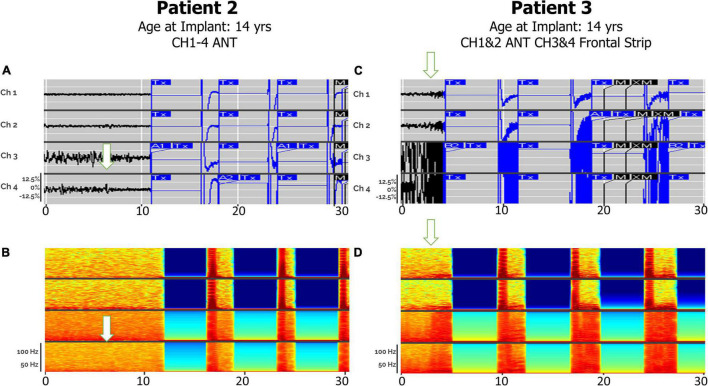
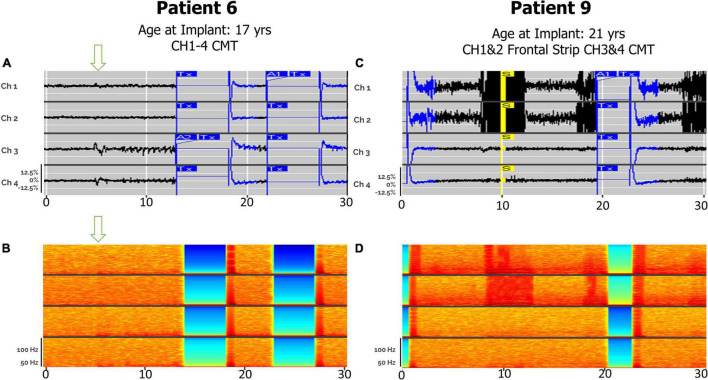
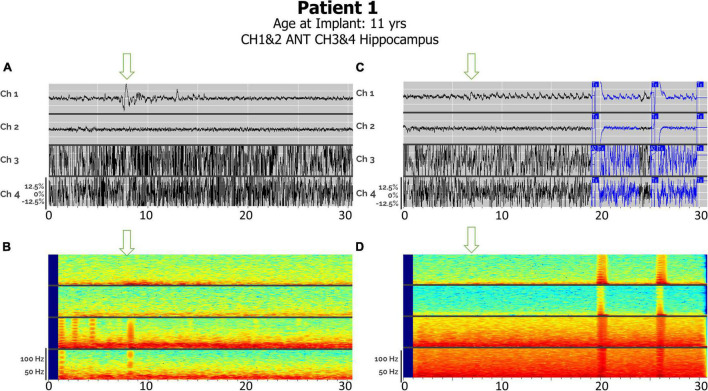
Anterior nucleus thalamic (ANT) leads, whether bilateral or unilateral and combined with a cortical strip lead, successfully detected and terminated epileptiform activity, as demonstrated by Cases 2 and 3. Similarly, bilateral centromedian thalamic (CMT) leads or a combination of one centromedian thalamic alongside a cortical strip lead also demonstrated the ability to detect electrographic seizures as seen in Cases 6 and 9. Bilateral pulvinar leads likewise produced reliable seizure detection in Patient 14. Detections of electrographic seizures in thalamic nuclei did not appear to be affected by whether the patient was pediatric or adult at the time of RNS System implantation. Sole thalamic leads paralleled the combination of thalamic and cortical strip leads in terms of preventing the propagation of electrographic seizures.
Thalamic nuclei present a promising target for detection and stimulation via the RNS System for seizures with multifocal or generalized onsets. These areas provide a modifiable, reversible therapeutic option for patients who are not candidates for surgical resection or ablation.
响应性神经刺激(RNS系统)已被用作治疗顽固性癫痫的方法。RNS系统通过覆盖癫痫病灶的电极导线,对检测到的异常活动做出响应,对预先定义的癫痫样活动进行检测,并进行刺激,目的是降低癫痫发作的频率和严重程度。虽然丘脑电极导线通常与皮质条带电极导线联合植入,但单独使用双侧丘脑电极导线进行植入和刺激的情况较少见,且使用RNS系统丘脑电极导线检测脑电图癫痫发作的能力尚不确定。
本研究回顾性评估了14例植入了RNS系统丘脑深度电极导线的患者,这些患者有或没有同时植入皮质条带电极导线,以确定在丘脑中检测脑电图癫痫发作的能力。详细的患者情况和电极导线轨迹与脑电图(ECoG)分析一起进行了回顾。
丘脑前核(ANT)电极导线,无论是双侧还是单侧,并与皮质条带电极导线联合使用,都成功检测并终止了癫痫样活动,如病例2和病例3所示。同样,双侧中央中核(CMT)电极导线或一根中央中核电极导线与皮质条带电极导线的组合也显示出检测脑电图癫痫发作的能力,如病例6和病例9所示。双侧枕核电极导线同样在患者14中产生了可靠的癫痫发作检测。在丘脑核中检测脑电图癫痫发作似乎不受患者在植入RNS系统时是儿童还是成人的影响。单独的丘脑电极导线在预防脑电图癫痫发作的传播方面与丘脑和皮质条带电极导线的组合相当。
丘脑核是通过RNS系统检测和刺激多灶性或全身性发作癫痫的一个有前景的靶点。这些区域为不适合手术切除或消融的患者提供了一种可调节、可逆的治疗选择。