Saharia Kapil K, Husson Jennifer S, Niederhaus Silke V, Iraguha Thierry, Avila Stephanie V, Yoo Youngchae J, Hardy Nancy M, Fan Xiaoxuan, Omili Destiny, Crane Alice, Carrier Amber, Xie Wen Y, Vander Mause Erica, Hankey Kim, Bauman Sherri, Lesho Patricia, Mannuel Heather D, Ahuja Ashish, Mathew Minu, Avruch James, Baddley John, Goloubeva Olga, Shetty Kirti, Dahiya Saurabh, Rapoport Aaron P, Luetkens Tim, Atanackovic Djordje
Institute of Human Virology University of Maryland School of Medicine Baltimore MD USA.
Divison of Infectious Diseases University of Maryland School of Medicine Baltimore MD USA.
Clin Transl Immunology. 2022 Apr 29;11(5):e1391. doi: 10.1002/cti2.1391. eCollection 2022.
Solid organ transplant recipients (SOTR) receiving post-transplant immunosuppression show increased COVID-19-related mortality. It is unclear whether an additional dose of COVID-19 vaccines can overcome the reduced immune responsiveness against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) variants.
We analysed humoral immune responses against SARS-CoV-2 and its variants in 53 SOTR receiving SARS-CoV-2 vaccination.
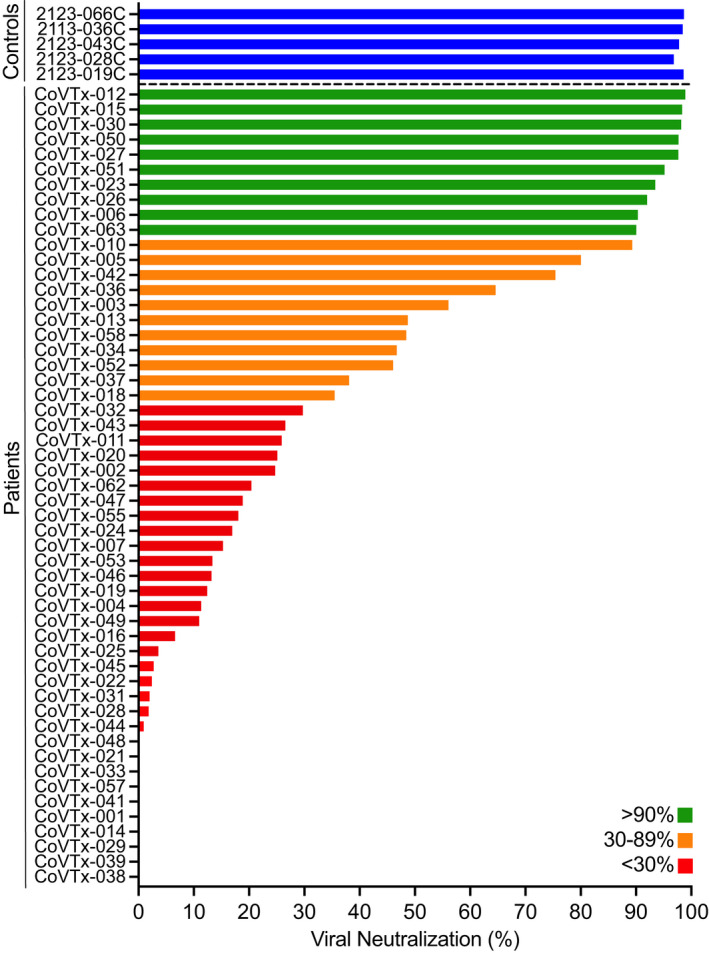
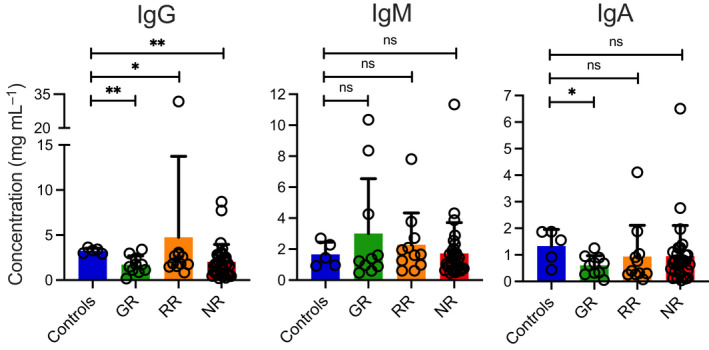
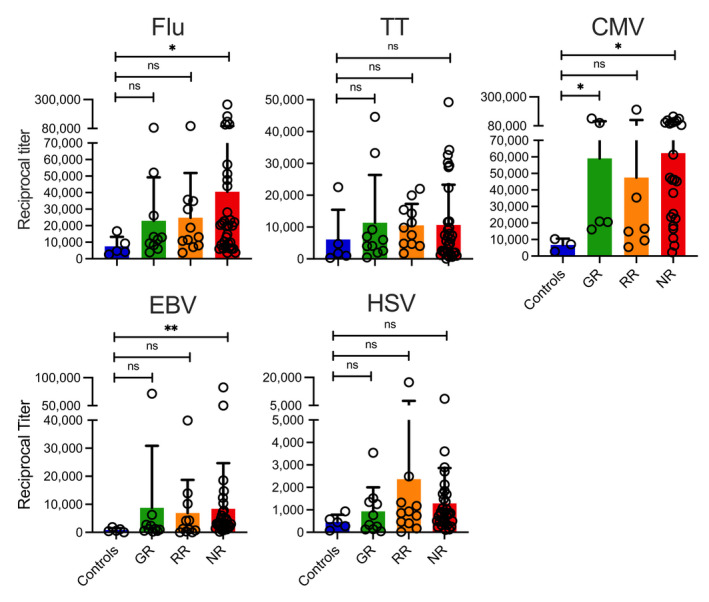
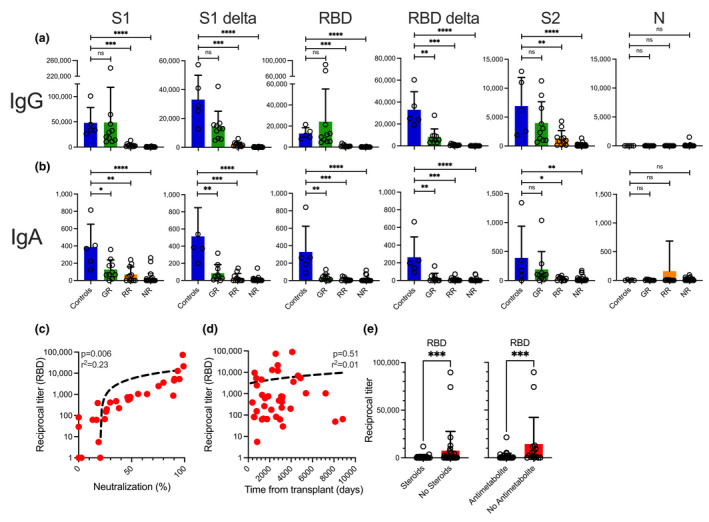
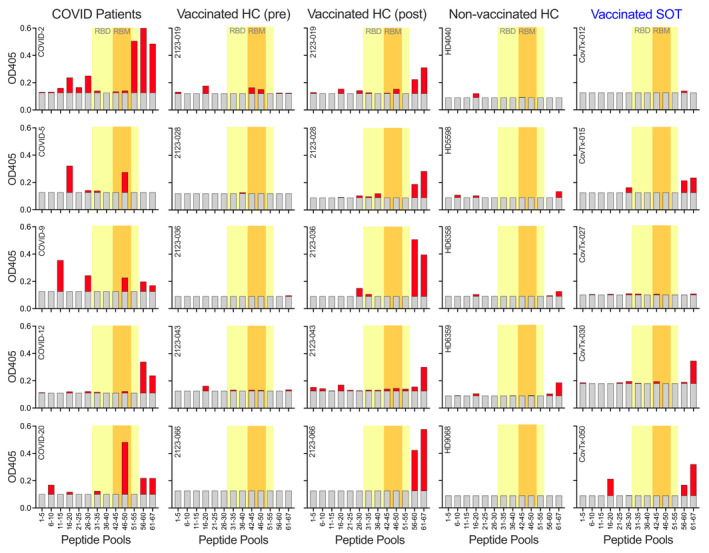
Following the initial vaccination series, 60.3% of SOTR showed no measurable neutralisation and only 18.9% demonstrated neutralising activity of > 90%. More intensive immunosuppression, antimetabolites in particular, negatively impacted antiviral immunity. While absolute IgG levels were lower in SOTR than controls, antibody titres against microbial recall antigens were higher. By contrast, SOTR showed reduced vaccine-induced IgG/IgA antibody titres against SARS-CoV-2 and its delta variants and fewer linear B-cell epitopes, indicating reduced B-cell diversity. Importantly, a third vaccine dose led to an increase in anti-SARS-CoV-2 antibody titres and neutralising activity across alpha, beta and delta variants and to the induction of anti-SARS-CoV-2 CD4 T cells in a subgroup of patients analysed. By contrast, we observed significantly lower antibody titres after the third dose with the omicron variant compared to the ancestral SARS-CoV-2 and the improvement in neutralising activity was much less pronounced than for all the other variants.
Only a small subgroup of solid organ transplant recipients is able to generate functional antibodies after an initial vaccine series; however, an additional vaccine dose resulted in dramatically improved antibody responses against all SARS-CoV-2 variants except omicron where antibody responses and neutralising activity remained suboptimal.
接受移植后免疫抑制的实体器官移植受者(SOTR)显示出与2019冠状病毒病(COVID-19)相关的死亡率增加。尚不清楚额外一剂COVID-19疫苗是否能克服针对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)变体的免疫反应降低问题。
我们分析了53名接受SARS-CoV-2疫苗接种的SOTR对SARS-CoV-2及其变体的体液免疫反应。
在初始疫苗接种系列后,60.3%的SOTR显示无可测量的中和作用,只有18.9%表现出>90%的中和活性。更强化的免疫抑制,尤其是抗代谢物,对抗病毒免疫产生负面影响。虽然SOTR中的绝对免疫球蛋白G(IgG)水平低于对照组,但针对微生物回忆抗原的抗体滴度更高。相比之下,SOTR显示针对SARS-CoV-2及其德尔塔变体的疫苗诱导IgG/IgA抗体滴度降低,线性B细胞表位减少,表明B细胞多样性降低。重要的是,第三剂疫苗导致分析的亚组患者中针对阿尔法、贝塔和德尔塔变体的抗SARS-CoV-2抗体滴度和中和活性增加,并诱导产生抗SARS-CoV-2 CD4 T细胞。相比之下,与原始SARS-CoV-2相比,我们观察到接种第三剂后针对奥密克戎变体的抗体滴度显著降低,且中和活性的改善远不如所有其他变体明显。
只有一小部分实体器官移植受者在初始疫苗接种系列后能够产生功能性抗体;然而,额外一剂疫苗导致针对除奥密克戎以外的所有SARS-CoV-2变体的抗体反应显著改善,而针对奥密克戎的抗体反应和中和活性仍然欠佳。