Department of Pulmonary Medicine, Shanghai Chest Hospital, Shanghai Jiaotong University, Shanghai, 200030, China.
State Key Laboratory of Molecular Oncology, Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
BMC Med. 2022 May 5;20(1):170. doi: 10.1186/s12916-022-02360-x.
In non-small cell lung cancer (NSCLC) patients receiving immune checkpoint inhibitors (ICIs), higher blood tumor mutational burden (bTMB) was usually associated with better progression-free survival (PFS) and objective response rate (ORR). However, the association between bTMB and overall survival (OS) benefit remains undefined. It has been reported that patients harboring a high level of circulating tumor DNA (ctDNA) had poor survival. We hypothesized that ctDNA-adjusted bTMB might predict OS benefit in NSCLC patients receiving ICIs.
Our study was retrospectively performed in three cohorts, including OAK and POPLAR cohort (n = 853), Shanghai and Wuhan (SH&WH) cohort (n = 44), and National Cancer Center (NCC) cohort (n = 47). Durable clinical benefit (DCB) was defined as PFS lasting ≥ 6 months. The cutoff value of ctDNA-adjusted bTMB for DCB prediction was calculated based on a receiver operating characteristic curve. Interaction between treatments and ctDNA-adjusted bTMB was assessed.
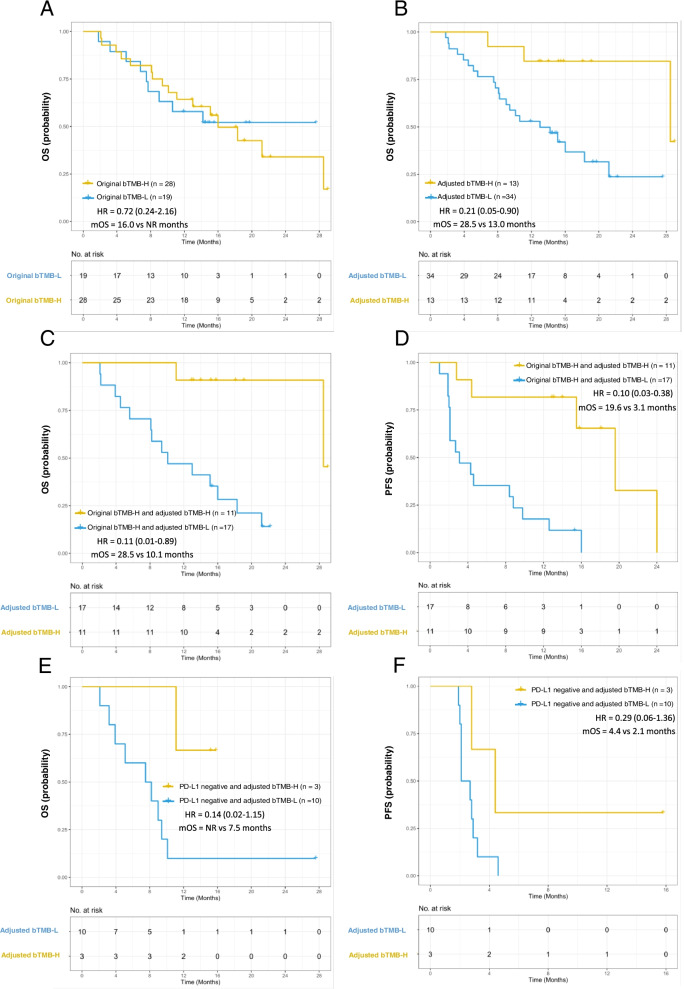
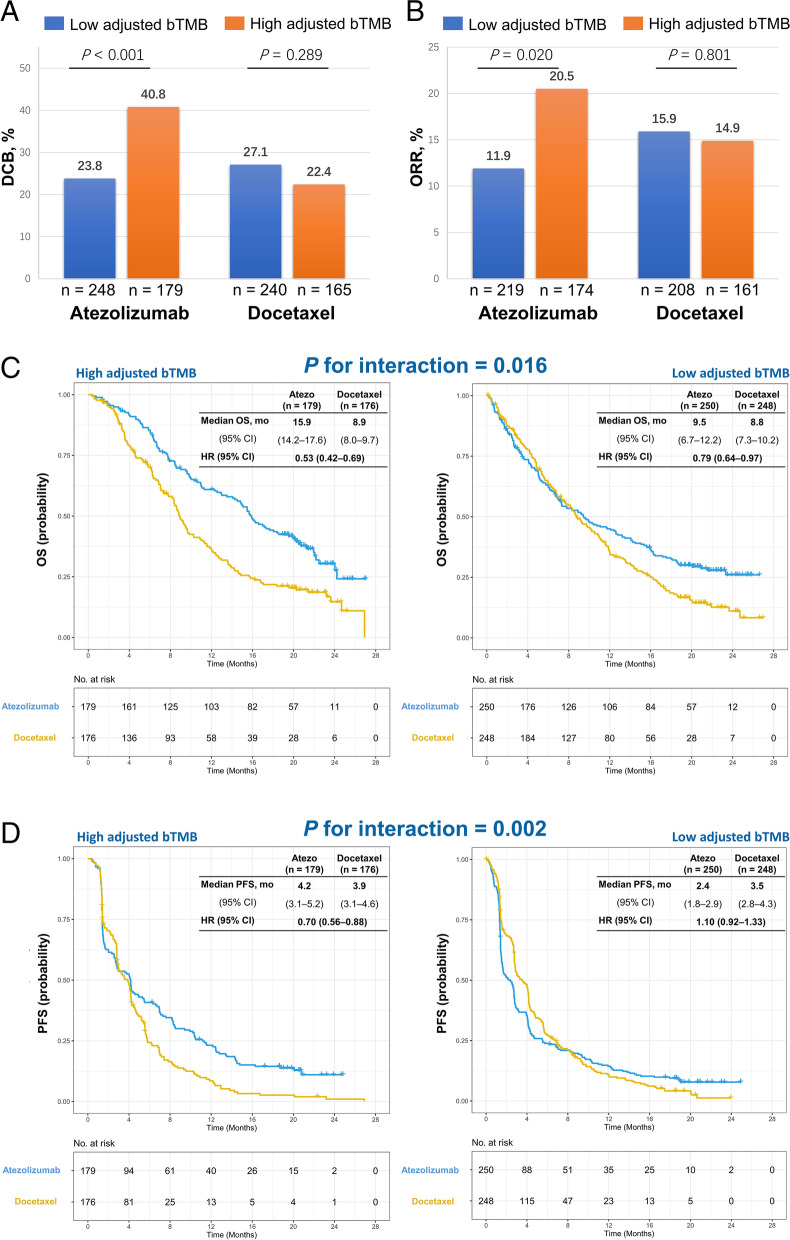
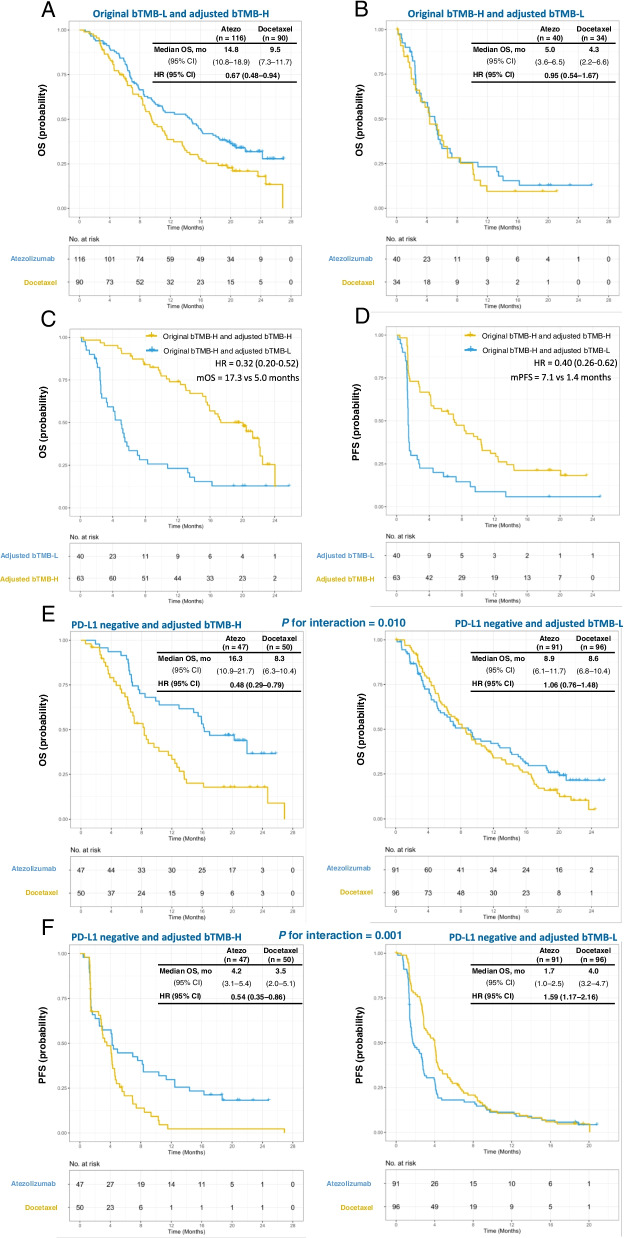
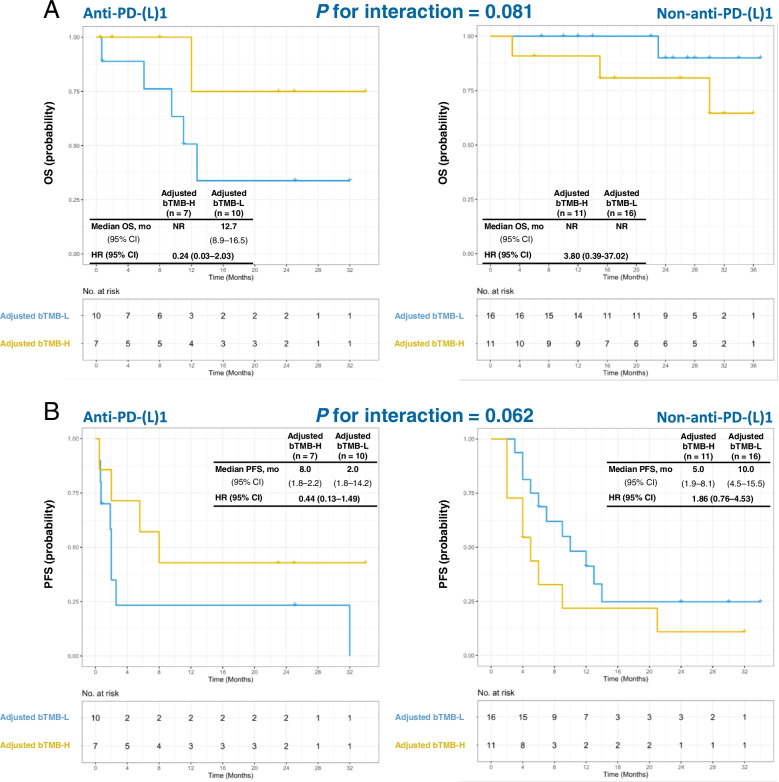
The bTMB score was significantly associated with tumor burden, while no association was observed between ctDNA-adjusted bTMB with tumor burden. In the OAK and POPLAR cohort, significantly higher ORR (P = 0.020) and DCB (P < 0.001) were observed in patients with high ctDNA-adjusted bTMB than those with low ctDNA-adjusted bTMB. Importantly, the interactions between ctDNA-adjusted bTMB and treatments were significant for OS (interaction P = 0.019) and PFS (interaction P = 0.002). In the SH&WH cohort, the interactions between ctDNA-adjusted bTMB and treatment were marginally significant for OS (interaction P = 0.081) and PFS (interaction P = 0.062). Similar result was demonstrated in the NCC cohort.
Our study indicated that ctDNA-adjusted bTMB might predict OS benefit in NSCLC patients receiving ICIs. The potential of ctDNA-adjusted bTMB as a noninvasive predictor for immunotherapy should be confirmed in future studies.
在接受免疫检查点抑制剂(ICI)治疗的非小细胞肺癌(NSCLC)患者中,较高的血液肿瘤突变负担(bTMB)通常与更好的无进展生存期(PFS)和客观缓解率(ORR)相关。然而,bTMB 与总生存期(OS)获益之间的关系尚未确定。据报道,携带高水平循环肿瘤 DNA(ctDNA)的患者生存情况较差。我们假设 ctDNA 调整后的 bTMB 可能预测接受 ICI 治疗的 NSCLC 患者的 OS 获益。
我们的研究在三个队列中进行了回顾性分析,包括 OAK 和 POPLAR 队列(n=853)、上海和武汉(SH&WH)队列(n=44)和国家癌症中心(NCC)队列(n=47)。持久临床获益(DCB)定义为 PFS 持续时间≥6 个月。基于受试者工作特征曲线计算用于预测 DCB 的 ctDNA 调整后 bTMB 的截止值。评估了治疗方法与 ctDNA 调整后 bTMB 之间的相互作用。
bTMB 评分与肿瘤负担显著相关,而 ctDNA 调整后的 bTMB 与肿瘤负担之间没有相关性。在 OAK 和 POPLAR 队列中,高 ctDNA 调整后 bTMB 的患者比低 ctDNA 调整后 bTMB 的患者具有更高的客观缓解率(P=0.020)和 DCB(P<0.001)。重要的是,ctDNA 调整后 bTMB 与治疗方法之间的相互作用对 OS(交互 P=0.019)和 PFS(交互 P=0.002)具有显著意义。在 SH&WH 队列中,ctDNA 调整后 bTMB 与治疗方法之间的相互作用对 OS(交互 P=0.081)和 PFS(交互 P=0.062)有边缘显著意义。在 NCC 队列中也得到了类似的结果。
本研究表明,ctDNA 调整后的 bTMB 可能预测接受 ICI 治疗的 NSCLC 患者的 OS 获益。ctDNA 调整后的 bTMB 作为免疫治疗的非侵入性预测因子的潜力需要在未来的研究中得到证实。