Wang Yu, Wang Wenqing, Zhang Tao, Yang Yin, Wang Jianyang, Li Canjun, Xu Xin, Wu Yuqi, Jiang Ying, Duan Jinghao, Wang Luhua, Bi Nan
Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
Department of Radiation Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, China.
J Natl Cancer Cent. 2024 Apr 10;4(2):177-187. doi: 10.1016/j.jncc.2024.01.008. eCollection 2024 Jun.
Liquid biopsy-based biomarkers, including circulating tumor DNA (ctDNA) and blood tumor mutational burden (bTMB), are recognized as promising predictors of prognoses and responses to immune checkpoint inhibitors (ICIs), despite insufficient sensitivity of single biomarker detection. This research aims to determine whether the combinatorial utility of longitudinal ctDNA with bTMB analysis could improve the prognostic and predictive effects.
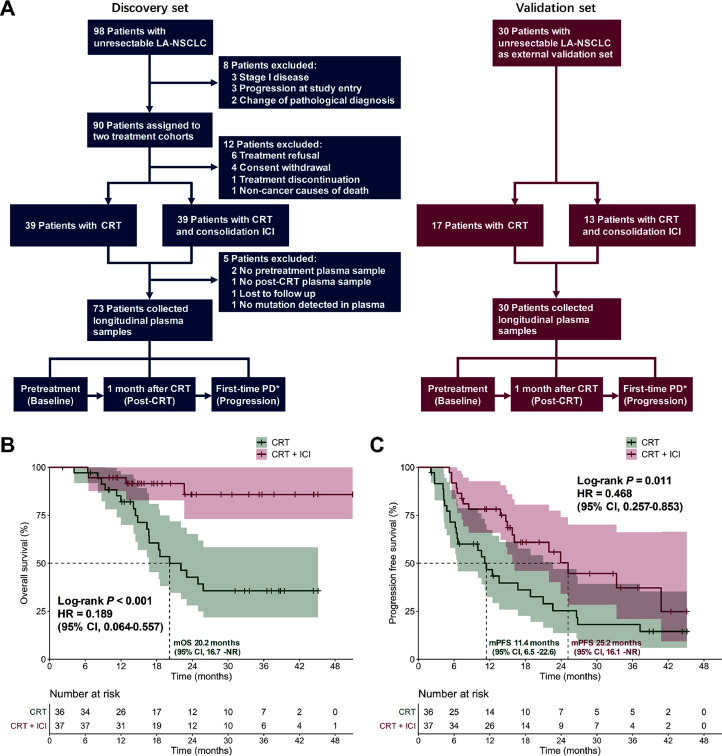
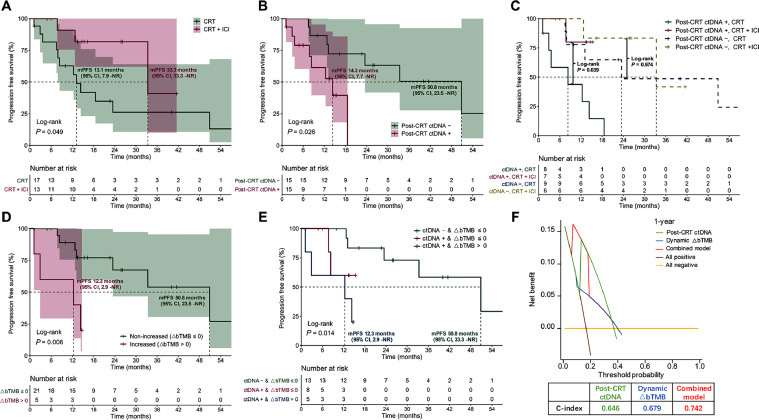
This prospective two-center cohort trial, consisting of discovery and validation datasets, enrolled unresectable locally advanced non-small-cell lung cancer (LA-NSCLC) patients and assigned them to chemoradiotherapy (CRT) or CRT + consolidation ICI cohorts from 2018 to 2022. Blood specimens were collected pretreatment, 4 weeks post-CRT, and at progression to assess bTMB and ctDNA using 486-gene next-generation sequencing. Dynamic ∆bTMB was calculated as post-CRT bTMB minus baseline bTMB levels. Decision curve analyses were performed to calculate Concordance index (C-index).
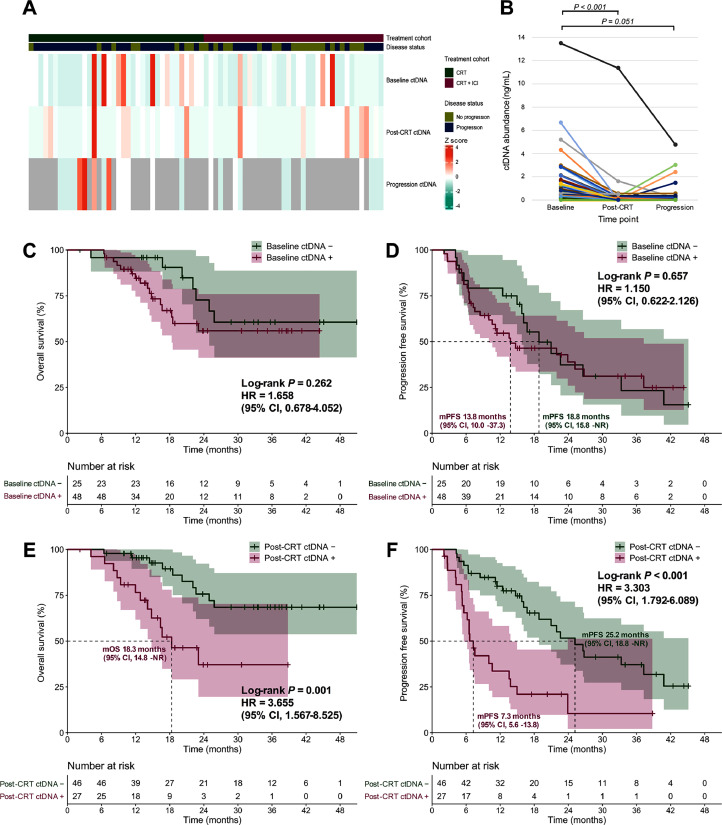
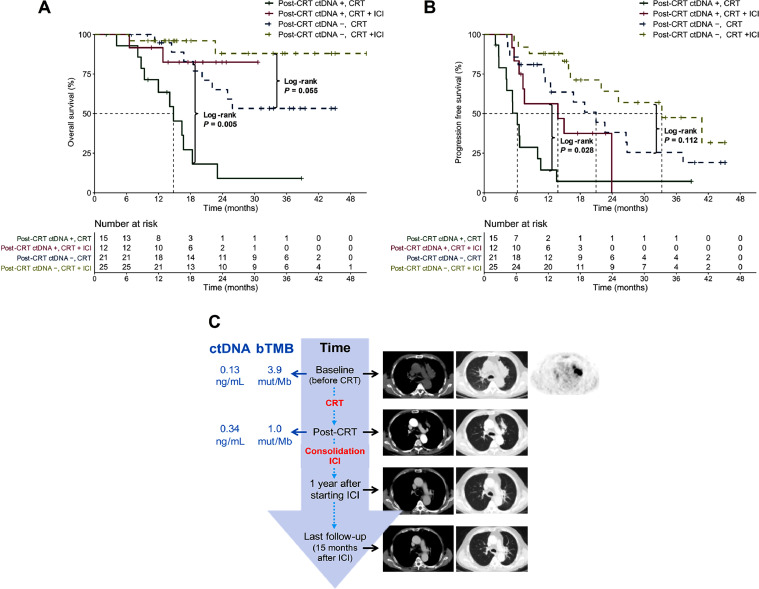
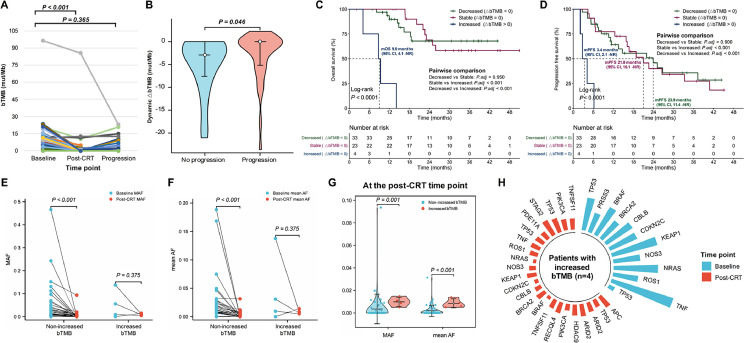
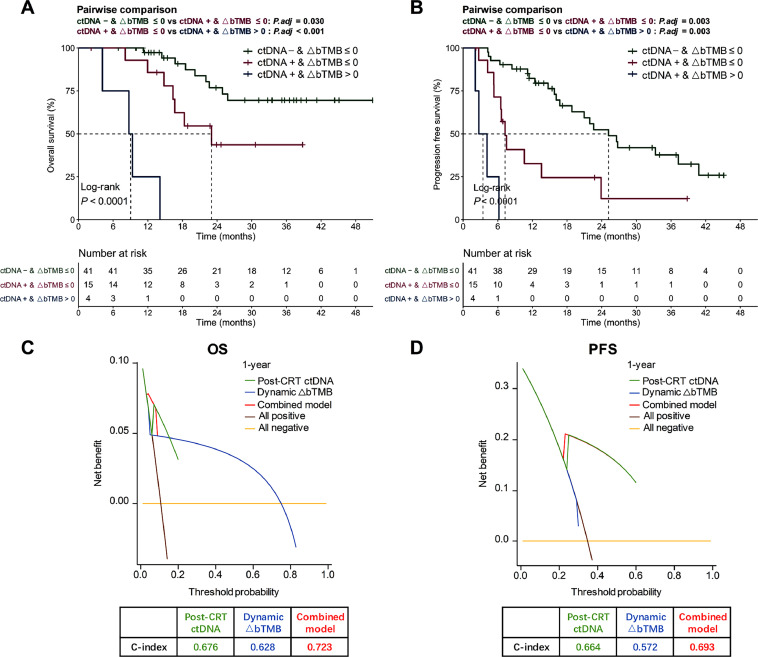
One hundred twenty-eight patients were enrolled. In the discovery dataset ( = 73), patients treated with CRT and consolidation ICI had significantly longer overall survival (OS; median not reached [NR] vs 20.2 months; < 0.001) and progression-free survival (PFS; median 25.2 vs 11.4 months; = 0.011) than those without ICI. Longitudinal analysis demonstrated a significant decrease in ctDNA abundance post-CRT ( < 0.001) but a relative increase with disease progression. Post-CRT detectable residual ctDNA correlated with significantly shorter OS (median 18.3 months vs NR; = 0.001) and PFS (median 7.3 vs 25.2 months; < 0.001). For patients with residual ctDNA, consolidation ICI brought significantly greater OS (median NR vs 14.8 months; = 0.005) and PFS (median 13.8 vs 6.2 months; = 0.028) benefit, but no significant difference for patients with ctDNA clearance. Dynamic ∆bTMB was predictive of prognosis. Patients with residual ctDNA and increased ∆bTMB (∆bTMB > 0) had significantly worse OS (median 9.0 vs 23.0 months vs NR; < 0.001) and PFS (median 3.4 vs 7.3 vs 25.2 months; < 0.001). The combinatorial model integrating post-CRT ctDNA with ∆bTMB had optimal predictive effects on OS (C-index = 0.723) and PFS (C-index = 0.693), outperforming individual features. In the independent validation set, we confirmed residual ctDNA predicted poorer PFS (median 50.8 vs 14.3 months; = 0.026) but identified more consolidation ICI benefit (median NR vs 8.3 months; = 0.039). The combined model exhibited a stable predictive advantage (C-index = 0.742 for PFS).
The multiparameter assay integrating qualitative residual ctDNA testing with quantitative ∆bTMB dynamics improves patient prognostic risk stratification and efficacy predictions, allowing for personalized consolidation therapy for LA-NSCLC.
基于液体活检的生物标志物,包括循环肿瘤DNA(ctDNA)和血液肿瘤突变负荷(bTMB),尽管单一生物标志物检测的敏感性不足,但仍被认为是预后和免疫检查点抑制剂(ICI)反应的有前景的预测指标。本研究旨在确定纵向ctDNA与bTMB分析的联合应用是否能提高预后和预测效果。
这项前瞻性双中心队列试验由发现和验证数据集组成,纳入了不可切除的局部晚期非小细胞肺癌(LA-NSCLC)患者,并在2018年至2022年将他们分配到放化疗(CRT)或CRT+巩固ICI队列。在治疗前、CRT后4周和疾病进展时采集血样,使用486基因下一代测序评估bTMB和ctDNA。动态∆bTMB计算为CRT后bTMB减去基线bTMB水平。进行决策曲线分析以计算一致性指数(C指数)。
共纳入128例患者。在发现数据集中(n=73),接受CRT和巩固ICI治疗的患者的总生存期(OS;中位未达到[NR] vs 20.2个月;P<0.001)和无进展生存期(PFS;中位25.2 vs 11.4个月;P=0.011)显著长于未接受ICI治疗的患者。纵向分析显示,CRT后ctDNA丰度显著降低(P<0.001),但随疾病进展相对增加。CRT后可检测到的残留ctDNA与显著缩短的OS(中位18.3个月vs NR;P=0.001)和PFS(中位7.3 vs 25.2个月;P<0.001)相关。对于残留ctDNA的患者,巩固ICI带来显著更大的OS(中位NR vs 14.8个月;P=0.005)和PFS(中位13.8 vs 6.2个月;P=0.028)获益,但对于ctDNA清除的患者无显著差异。动态∆bTMB可预测预后。残留ctDNA且∆bTMB增加(∆bTMB>0)的患者的OS(中位9.0 vs 23.0个月vs NR;P<0.001)和PFS(中位3.4 vs 7.3 vs 25.2个月;P<0.001)显著更差。将CRT后ctDNA与∆bTMB整合的联合模型对OS(C指数=0.723)和PFS(C指数=0.693)具有最佳预测效果,优于个体特征。在独立验证集中,我们证实残留ctDNA预测较差的PFS(中位50.8 vs 14.3个月;P=0.026),但发现更多巩固ICI的获益(中位NR vs 8.3个月;P=0.039)。联合模型表现出稳定的预测优势(PFS的C指数=0.742)。
将定性残留ctDNA检测与定量∆bTMB动态分析相结合的多参数检测可改善患者预后风险分层和疗效预测,为LA-NSCLC患者提供个性化的巩固治疗。