Center for Convergent Research for Emerging Virus Infection, Korea Research Institute of Chemical Technologygrid.29869.3c, Daejeon, Republic of Korea.
Arontier Co., Ltd., Seoul, Republic of Korea.
Microbiol Spectr. 2022 Jun 29;10(3):e0109122. doi: 10.1128/spectrum.01091-22. Epub 2022 May 5.
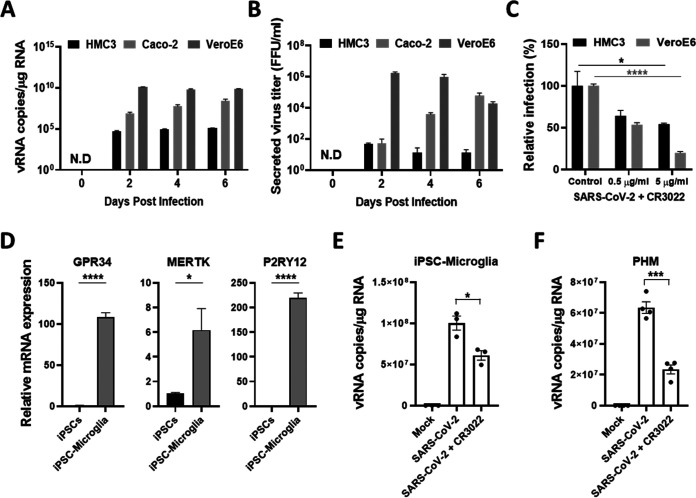
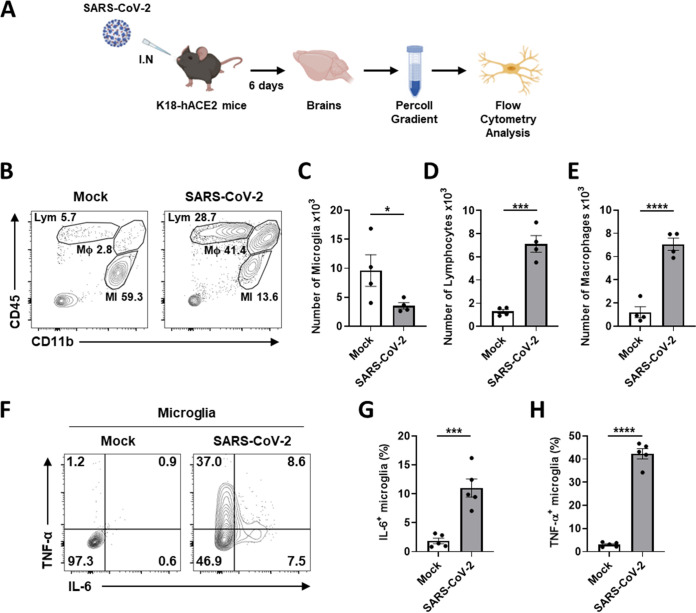
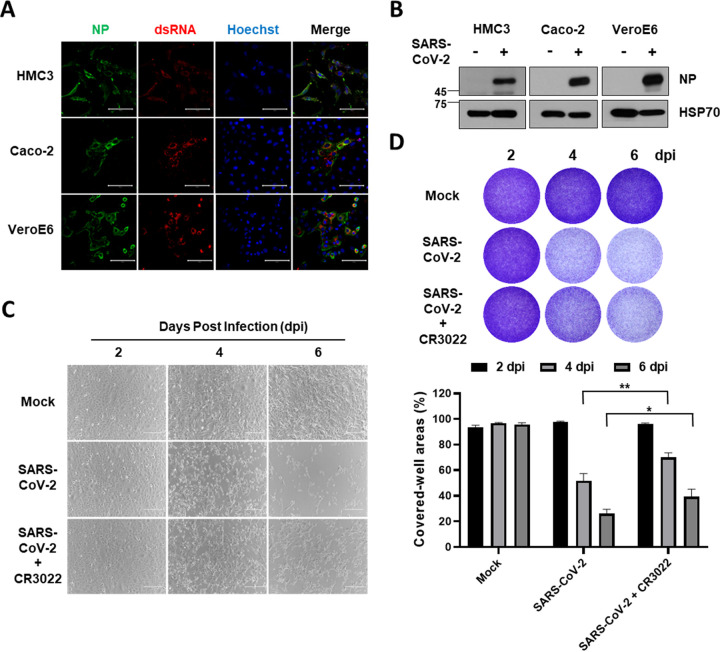
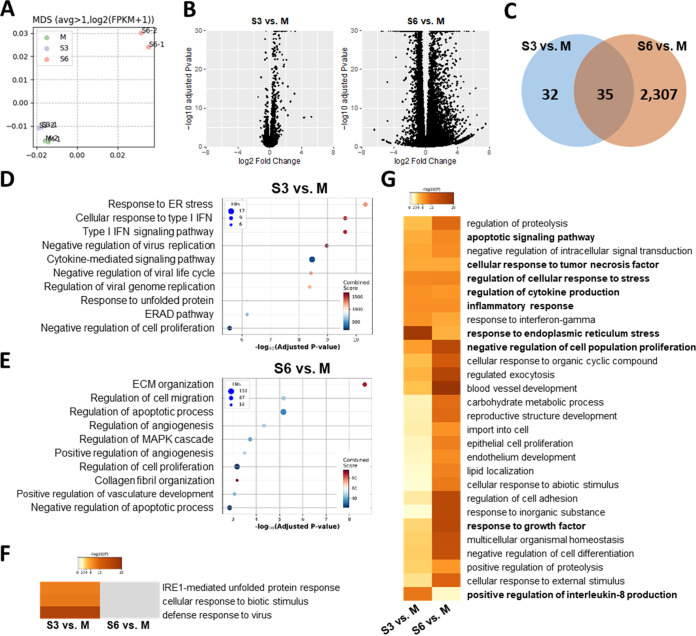
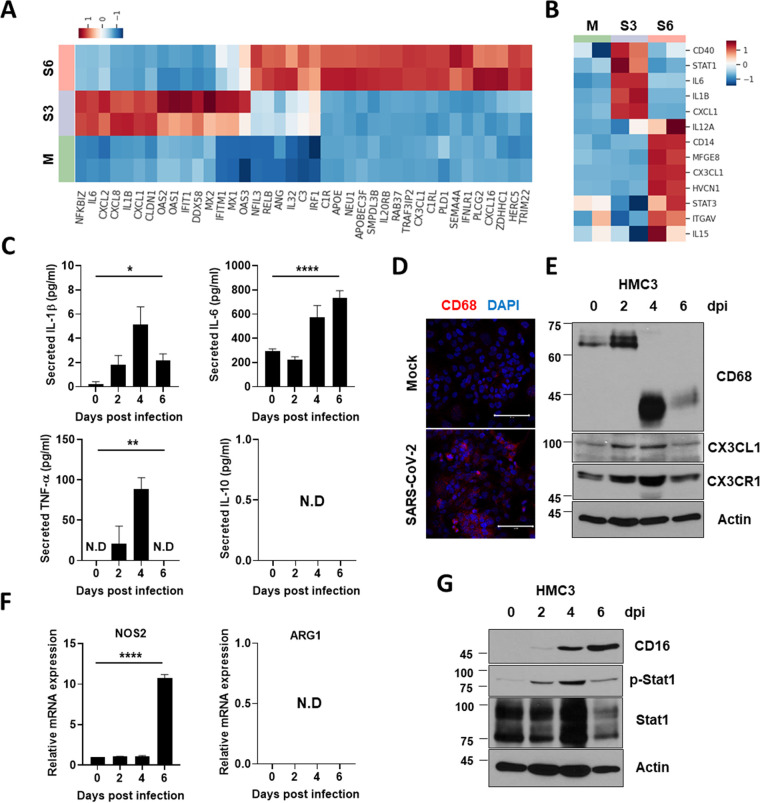
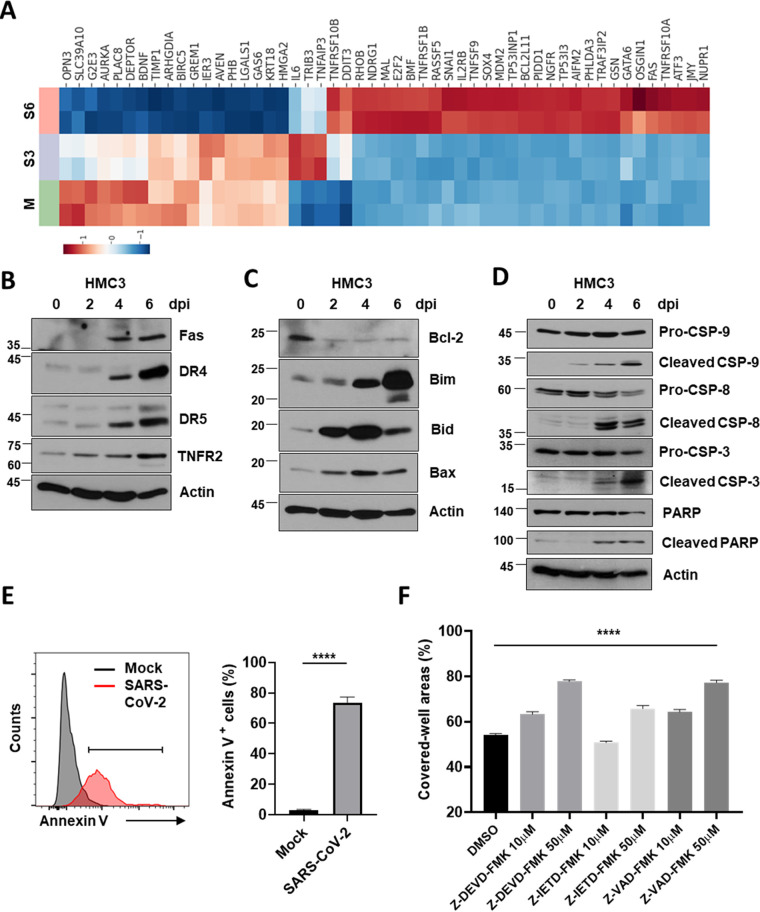
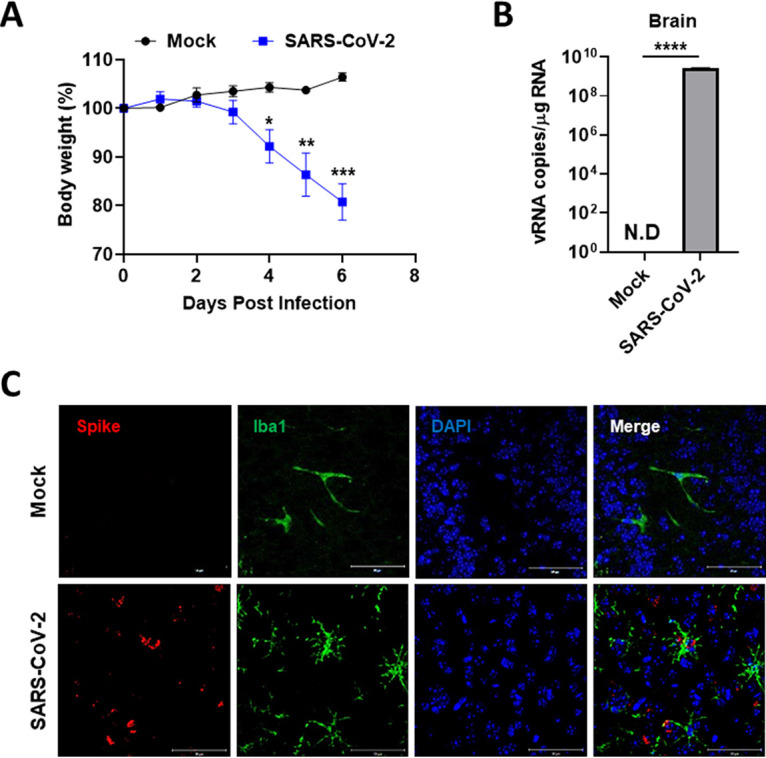
Accumulating evidence suggests that severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection causes various neurological symptoms in patients with coronavirus disease 2019 (COVID-19). The most dominant immune cells in the brain are microglia. Yet, the relationship between neurological manifestations, neuroinflammation, and host immune response of microglia to SARS-CoV-2 has not been well characterized. Here, we reported that SARS-CoV-2 can directly infect human microglia, eliciting M1-like proinflammatory responses, followed by cytopathic effects. Specifically, SARS-CoV-2 infected human microglial clone 3 (HMC3), leading to inflammatory activation and cell death. RNA sequencing (RNA-seq) analysis also revealed that endoplasmic reticulum (ER) stress and immune responses were induced in the early, and apoptotic processes in the late phases of viral infection. SARS-CoV-2-infected HMC3 showed the M1 phenotype and produced proinflammatory cytokines, such as interleukin (IL)-1β, IL-6, and tumor necrosis factor α (TNF-α), but not the anti-inflammatory cytokine IL-10. After this proinflammatory activation, SARS-CoV-2 infection promoted both intrinsic and extrinsic death receptor-mediated apoptosis in HMC3. Using K18-hACE2 transgenic mice, murine microglia were also infected by intranasal inoculation of SARS-CoV-2. This infection induced the acute production of proinflammatory microglial IL-6 and TNF-α and provoked a chronic loss of microglia. Our findings suggest that microglia are potential mediators of SARS-CoV-2-induced neurological problems and, consequently, can be targets of therapeutic strategies against neurological diseases in patients with COVID-19. Recent studies reported neurological and cognitive sequelae in patients with COVID-19 months after the viral infection with several symptoms, including ageusia, anosmia, asthenia, headache, and brain fog. Our conclusions raise awareness of COVID-19-related microglia-mediated neurological disorders to develop treatment strategies for the affected patients. We also indicated that HMC3 was a novel human cell line susceptible to SARS-CoV-2 infection that exhibited cytopathic effects, which could be further used to investigate cellular and molecular mechanisms of neurological manifestations of patients with COVID-19.
越来越多的证据表明,严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)感染会导致 2019 冠状病毒病(COVID-19)患者出现各种神经系统症状。大脑中最主要的免疫细胞是小胶质细胞。然而,神经系统表现、神经炎症以及小胶质细胞对 SARS-CoV-2 的宿主免疫反应之间的关系尚未得到很好的描述。在这里,我们报道了 SARS-CoV-2 可以直接感染人小胶质细胞,引发 M1 样促炎反应,随后产生细胞病变效应。具体来说,SARS-CoV-2 感染人小胶质细胞克隆 3(HMC3),导致炎症激活和细胞死亡。RNA 测序(RNA-seq)分析还显示,病毒感染的早期诱导内质网(ER)应激和免疫反应,晚期诱导凋亡过程。SARS-CoV-2 感染的 HMC3 表现出 M1 表型,并产生促炎细胞因子,如白细胞介素(IL)-1β、IL-6 和肿瘤坏死因子-α(TNF-α),但不产生抗炎细胞因子 IL-10。在这种促炎激活之后,SARS-CoV-2 感染促进了 HMC3 中内在和外在死亡受体介导的细胞凋亡。使用 K18-hACE2 转基因小鼠,通过鼻腔接种 SARS-CoV-2 也感染了鼠小胶质细胞。这种感染诱导了促炎小胶质细胞 IL-6 和 TNF-α 的急性产生,并导致小胶质细胞慢性丧失。我们的研究结果表明,小胶质细胞可能是 SARS-CoV-2 引起的神经问题的潜在介质,因此可以成为针对 COVID-19 患者神经疾病的治疗策略的靶点。最近的研究报告称,在病毒感染数月后,COVID-19 患者出现了包括味觉丧失、嗅觉丧失、乏力、头痛和脑雾在内的神经系统和认知后遗症。我们的结论提高了对 COVID-19 相关小胶质细胞介导的神经紊乱的认识,以制定针对受影响患者的治疗策略。我们还表明,HMC3 是一种对 SARS-CoV-2 感染敏感的新型人细胞系,表现出细胞病变效应,可进一步用于研究 COVID-19 患者神经系统表现的细胞和分子机制。