Colorectal Surgery and Oncology, Key Laboratory of Cancer Prevention and Intervention, Ministry of Education, The Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, China.
Medical Oncology, The Second Affiliated Hospital of Zhejiang University School of Medicine, Hangzhou, China.
BMC Med. 2022 May 6;20(1):155. doi: 10.1186/s12916-022-02357-6.
Anlotinib, an oral small molecule tyrosine kinase inhibitor targeting VEGFR 1/2/3, FGFR 1-4, PDGFR a/β, and c-kit, had demonstrated prolonged progression-free survival (PFS) in refractory metastatic colorectal cancer (mCRC). This multicenter, single-arm, phase II, exploratory study was conducted to evaluate the efficacy and safety of anlotinib combined with capecitabine and oxaliplatin as first-line treatment for unresectable RAS/BRAF wild-type mCRC.
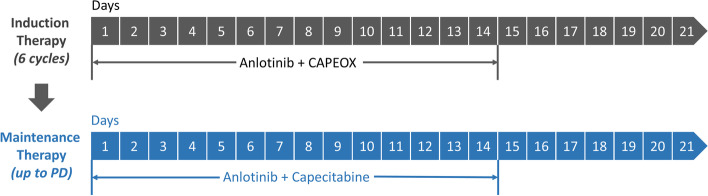
Patients aged 18-75 with RAS/BRAF wild-type unresectable mCRC, without prior systemic treatment, and ECOG performance status ≤1 were enrolled. Eligible patients received capecitabine (850 mg/m, p.o., bid, on day 1-14 every 21 days), oxaliplatin (130 mg/m, i.v., on day 1 every 21 days), and anlotinib (12 mg, p.o., qd, on days 1-14 every 21 days) as induction therapy. Following 6 cycles of therapy, patients who achieved response or stable disease received capecitabine and anlotinib as maintenance therapy until tumor progression. The primary endpoint was objective response rate (ORR) according to RECIST (version: 1.1), and the secondary endpoints were PFS, disease control rate (DCR), duration of response (DOR), and safety.
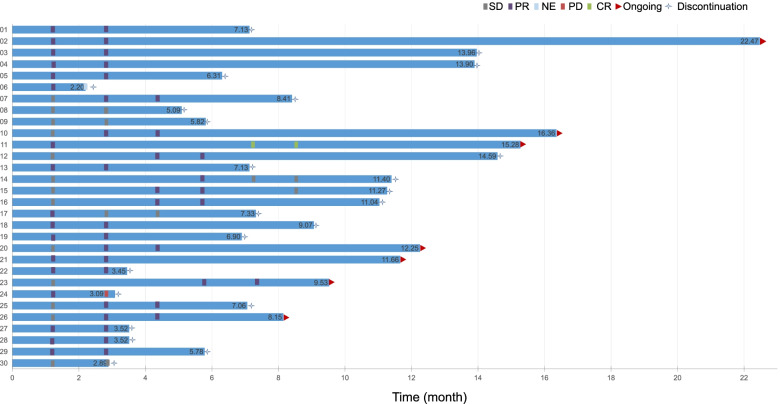
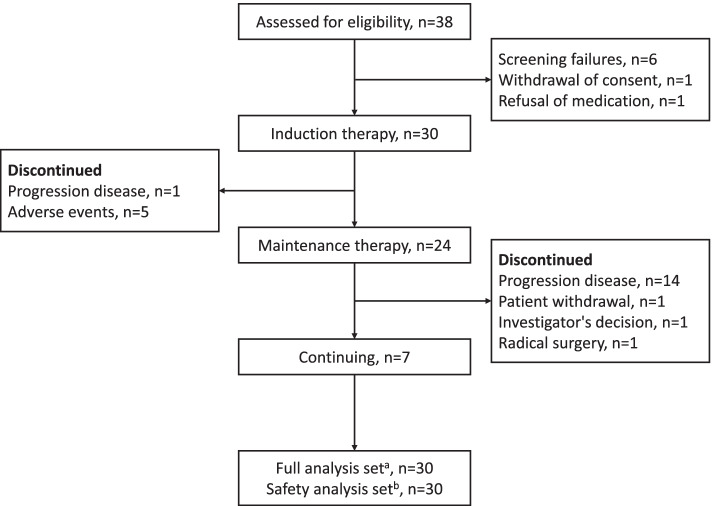
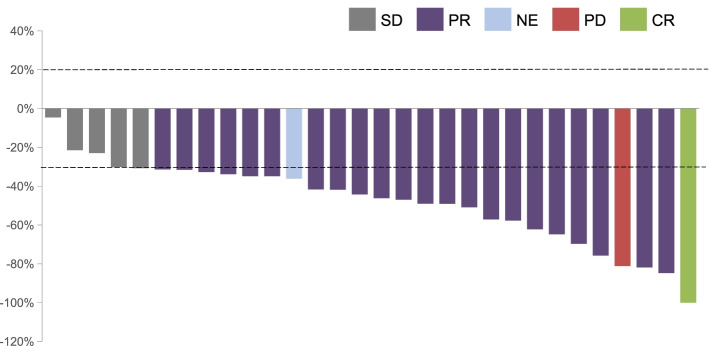
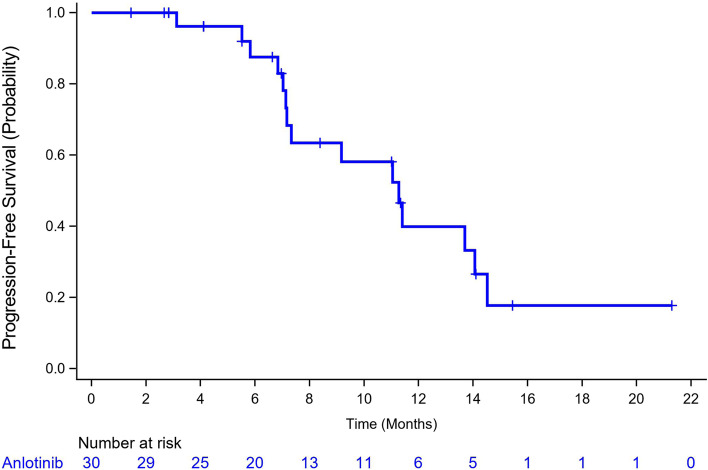
Between November 2019 and February 2021, 31 patients were enrolled. One patient was excluded for refusing treatment. The primary endpoint of ORR was 76.7% (95% CI, 57.7-90.1) with 1 patient achieving a complete response and 22 patients partial response. DCR was 93.3% (95% CI, 77.9-99.2). At a median follow-up of 14.1 months (95% CI, 9.9-18.3), median PFS was 11.3 months (95% CI, 7.1-14.1), and DOR was 7.9 months (95% CI, 5.5-12.7). Twenty-five (83.3%) patients experienced grade 3 or 4 treatment-emergent adverse events (TEAEs). No grade 5 TEAE was reported. The most common grade 3 or 4 TEAEs (>10%) were hypertension (15/30; 50%), neutrophil count decreased (8/30; 26.7%), and diarrhea (4/30; 13.3%). A total of 18 (60%) patients had TEAEs that resulted in dose reduction, interruptions, or delays.
Anlotinib combined with capecitabine and oxaliplatin showed considerable ORR, DCR, PFS, and DOR in the first-line therapy of mCRC with manageable toxicity profiles.
ClinicalTrials.gov : NCT04080843.
安罗替尼是一种口服小分子酪氨酸激酶抑制剂,针对 VEGFR1/2/3、FGFR1-4、PDGFRα/β 和 c-kit,在难治性转移性结直肠癌(mCRC)中表现出延长的无进展生存期(PFS)。本多中心、单臂、II 期、探索性研究旨在评估安罗替尼联合卡培他滨和奥沙利铂作为不可切除 RAS/BRAF 野生型 mCRC 的一线治疗的疗效和安全性。
招募年龄在 18-75 岁、RAS/BRAF 野生型不可切除 mCRC、未经系统治疗且 ECOG 体能状态评分≤1 的患者。符合条件的患者接受卡培他滨(850 mg/m2,口服,bid,第 1-14 天,每 21 天一次)、奥沙利铂(130 mg/m2,静脉注射,第 1 天,每 21 天一次)和安罗替尼(12 mg,口服,qd,第 1-14 天,每 21 天一次)作为诱导治疗。在 6 个周期的治疗后,达到缓解或疾病稳定的患者接受卡培他滨和安罗替尼维持治疗,直到肿瘤进展。主要终点是根据 RECIST(版本:1.1)评估的客观缓解率(ORR),次要终点是 PFS、疾病控制率(DCR)、缓解持续时间(DOR)和安全性。
2019 年 11 月至 2021 年 2 月期间,共招募了 31 名患者。1 名患者因拒绝治疗而被排除。ORR 的主要终点为 76.7%(95%CI,57.7-90.1),其中 1 名患者完全缓解,22 名患者部分缓解。DCR 为 93.3%(95%CI,77.9-99.2)。中位随访 14.1 个月(95%CI,9.9-18.3)时,中位 PFS 为 11.3 个月(95%CI,7.1-14.1),DOR 为 7.9 个月(95%CI,5.5-12.7)。25(83.3%)名患者发生 3 级或 4 级治疗相关不良事件(TEAEs)。无 5 级 TEAE 报告。最常见的 3 级或 4 级 TEAEs(>10%)为高血压(15/30;50%)、中性粒细胞计数减少(8/30;26.7%)和腹泻(4/30;13.3%)。共有 18(60%)名患者因 TEAEs 导致剂量减少、中断或延迟。
安罗替尼联合卡培他滨和奥沙利铂在 RAS/BRAF 野生型 mCRC 的一线治疗中显示出可观的 ORR、DCR、PFS 和 DOR,且毒性谱可管理。
ClinicalTrials.gov:NCT04080843。