Li Qiangqiang, Zhang Chen, Wang Rong, Keller Bradley B, Gu Hong
Department of Pediatric Cardiology, Beijing Anzhen Hospital Capital Medical University Beijing China.
Center for Anesthesiology, Beijing Anzhen Hospital Capital Medical University Beijing China.
Pulm Circ. 2022 Apr 18;12(2):e12067. doi: 10.1002/pul2.12067. eCollection 2022 Apr.
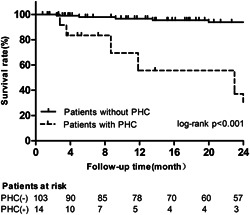
Pediatric patients with pulmonary arterial hypertension (PAH) are considered to be at risk for pulmonary hypertensive crisis (PHC) or even death during right heart catheterization (RHC). This retrospective study was designed to identify the risks and clinical characteristics associated with PHC in pediatric PAH patients. We included 163 consecutive procedures from 147 pediatric patients diagnosed with PAH who underwent diagnostic RHC in Beijing Anzhen Hospital between January 2007 and December 2020. The average patient age was 9.0 ± 4.7 years and 84 (51.5%) were females. Before RHC, over 20% of patients were in New York Heart Association (NYHA) class III-IV. Sedation or general intravenous anesthesia was used in 103 procedures (63.2%), with spontaneous breathing in 93.2%. PHC occurred in 19 patients (11.7%), 5 (3.1%) required cardiac compression, and 1 died (0.6%). Compared to patients without PHC, those who experienced PHC were more likely to be in NYHA class III-IV ( = 0.012) before RHC, require sedation ( = 0.011), had echocardiographic indices of higher peak tricuspid regurgitation velocity ( = 0.018), and right ventricle (RV) to left ventricle (LV) ratio ( < 0.001). Multivariate logistic regression for PHC identified the need for sedation and a higher RV/LV ratio as independent predictors. In conclusion, the risk of RHC remains significant in children with PAH, particularly in those with severe RV dilation who require sedation during cardiac catheterization. Comprehensive evaluation, close monitoring, and appropriate treatment before and during the procedure are essential for reducing mortality.
患有肺动脉高压(PAH)的儿科患者在右心导管检查(RHC)期间被认为有发生肺动脉高压危象(PHC)甚至死亡的风险。这项回顾性研究旨在确定儿科PAH患者中与PHC相关的风险和临床特征。我们纳入了2007年1月至2020年12月在北京安贞医院接受诊断性RHC的147例诊断为PAH的儿科患者的163例连续手术。患者平均年龄为9.0±4.7岁,84例(51.5%)为女性。在RHC之前,超过20%的患者处于纽约心脏协会(NYHA)III-IV级。103例手术(63.2%)使用了镇静或全身静脉麻醉,其中93.2%为自主呼吸。19例患者(11.7%)发生了PHC,5例(3.1%)需要心脏按压,1例死亡(0.6%)。与未发生PHC的患者相比,发生PHC的患者在RHC之前更可能处于NYHA III-IV级(P = 0.012),需要镇静(P = 0.011),有更高的三尖瓣反流峰值速度的超声心动图指标(P = 0.018)以及右心室(RV)与左心室(LV)比值(P < 0.001)。对PHC进行多因素逻辑回归分析发现,需要镇静和更高的RV/LV比值是独立预测因素。总之,PAH患儿进行RHC的风险仍然很大,特别是那些右心室严重扩张且在心脏导管检查期间需要镇静的患儿。术前和术中进行全面评估、密切监测和适当治疗对于降低死亡率至关重要。