Division of Cardiovascular Medicine, Department of Medicine, Beth Israel Deaconess Medical Center, Harvard Medical School, Boston, MA, USA.
Baim Institute for Clinical Research, Boston, MA, USA.
Curr Atheroscler Rep. 2022 Jul;24(7):585-597. doi: 10.1007/s11883-022-01025-7. Epub 2022 May 7.
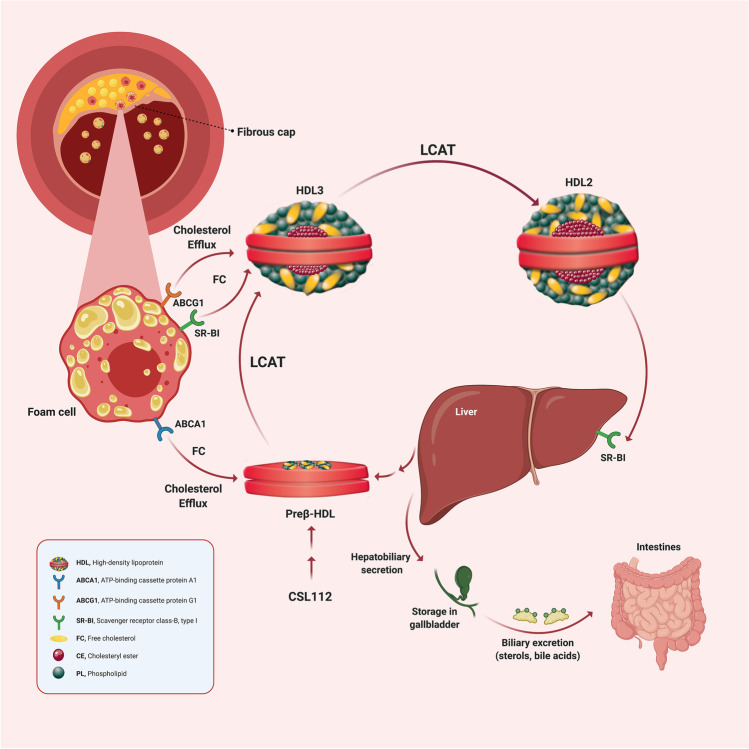
The elevated adverse cardiovascular event rate among patients with low high-density lipoprotein cholesterol (HDL-C) formed the basis for the hypothesis that elevating HDL-C would reduce those events. Attempts to raise endogenous HDL-C levels, however, have consistently failed to show improvements in cardiovascular outcomes. However, steady-state HDL-C concentration does not reflect the function of this complex family of particles. Indeed, HDL functions correlate only weakly with serum HDL-C concentration. Thus, the field has pivoted from simply raising the quantity of HDL-C to a focus on improving the putative anti-atherosclerotic functions of HDL particles. Such functions include the ability of HDL to promote the efflux of cholesterol from cholesterol-laden macrophages. Apolipoprotein A-I (apoA-I), the signature apoprotein of HDL, may facilitate the removal of cholesterol from atherosclerotic plaque, reduce the lesional lipid content and might thus stabilize vulnerable plaques, thereby reducing the risk of cardiac events. Infusion of preparations of apoA-I may improve cholesterol efflux capacity (CEC). This review summarizes the development of apoA-I therapies, compares their structural and functional properties and discusses the findings of previous studies including their limitations, and how CSL112, currently being tested in a phase III trial, may overcome these challenges.
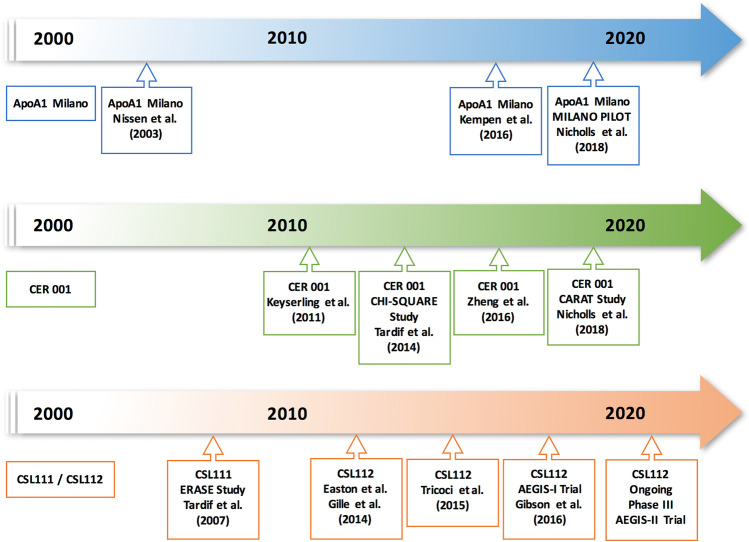
Three major ApoA-I-based approaches (MDCO-216, CER-001, and CSL111/CSL112) have aimed to enhance reverse cholesterol transport. These three therapies differ considerably in both lipid and protein composition. MDCO-216 contains recombinant ApoA-I Milano, CER-001 contains recombinant wild-type human ApoA-I, and CSL111/CSL112 contains native ApoA-I isolated from human plasma. Two of the three agents studied to date (apoA-1 Milano and CER-001) have undergone evaluation by intravascular ultrasound imaging, a technique that gauges lesion volume well but does not assess other important variables that may relate to clinical outcomes. ApoA-1 Milano and CER-001 reduce lecithin-cholesterol acyltransferase (LCAT) activity, potentially impairing the function of HDL in reverse cholesterol transport. Furthermore, apoA-I Milano can compete with and alter the function of the recipient's endogenous apoA-I. In contrast to these agents, CSL112, a particle formulated using human plasma apoA-I and phosphatidylcholine, increases LCAT activity and does not lead to the malfunction of endogenous apoA-I. CSL112 robustly increases cholesterol efflux, promotes reverse cholesterol transport, and now is being tested in a phase III clinical trial. Phase II-b studies of MDCO-216 and CER-001 failed to produce a significant reduction in coronary plaque volume as assessed by IVUS. However, the investigation to determine whether the direct infusion of a reconstituted apoA-I reduces post-myocardial infarction coronary events is being tested using CSL112, which is dosed at a higher level than MDCO-216 and CER-001 and has more favorable pharmacodynamics.
由于低高密度脂蛋白胆固醇(HDL-C)患者心血管不良事件发生率升高,因此假设升高 HDL-C 可降低这些事件的发生率。然而,尝试提高内源性 HDL-C 水平的方法并未显示出对心血管结局的改善。然而,稳态 HDL-C 浓度并不能反映这种复杂的 HDL 颗粒家族的功能。事实上,HDL 功能与血清 HDL-C 浓度的相关性很弱。因此,该领域已从单纯提高 HDL-C 的数量转向关注提高 HDL 颗粒的假定抗动脉粥样硬化功能。这种功能包括 HDL 促进载脂蛋白 B 胆固醇从载脂蛋白 B 胆固醇负荷巨噬细胞中流出的能力。载脂蛋白 A-I(apoA-I)是 HDL 的标志性载脂蛋白,可能有助于从动脉粥样硬化斑块中去除胆固醇,减少病变中的脂质含量,从而稳定易损斑块,从而降低心脏事件的风险。apoA-I 制剂的输注可能会改善胆固醇流出能力(CEC)。本综述总结了 apoA-I 治疗的发展,比较了它们的结构和功能特性,并讨论了以前研究的结果,包括它们的局限性,以及目前正在进行 III 期试验的 CSL112 如何克服这些挑战。
三种主要的基于 ApoA-I 的方法(MDCO-216、CER-001 和 CSL111/CSL112)旨在增强胆固醇逆转运。这三种疗法在脂质和蛋白质组成上有很大的不同。MDCO-216 含有重组 ApoA-I 米兰,CER-001 含有重组野生型人 ApoA-I,CSL111/CSL112 含有从人血浆中分离的天然 ApoA-I。迄今为止研究的两种(apoA-1 米兰和 CER-001)已经接受了血管内超声成像的评估,该技术很好地评估了病变体积,但不能评估可能与临床结果相关的其他重要变量。apoA-1 米兰和 CER-001 降低卵磷脂胆固醇酰基转移酶(LCAT)活性,可能损害 HDL 在胆固醇逆转运中的功能。此外,apoA-I 米兰可以与并改变受者内源性 apoA-I 的功能。与这些药物相反,CSL112,一种使用人血浆 apoA-I 和磷脂酰胆碱制成的颗粒,增加了 LCAT 活性,不会导致内源性 apoA-I 功能障碍。CSL112 可显著增加胆固醇流出,促进胆固醇逆转运,目前正在进行 III 期临床试验。MDCO-216 和 CER-001 的 II-b 期研究未能如 IVUS 评估的那样显著减少冠状动脉斑块体积。然而,正在使用 CSL112 测试直接输注重组 apoA-I 是否会减少心肌梗死后的冠状动脉事件,CSL112 的剂量高于 MDCO-216 和 CER-001,并且具有更有利的药代动力学。