Boekel Laura, Stalman Eileen W, Wieske Luuk, Hooijberg Femke, van Dam Koos P J, Besten Yaëlle R, Kummer Laura Y L, Steenhuis Maurice, van Kempen Zoé L E, Killestein Joep, Volkers Adriaan G, Tas Sander W, van der Kooi Anneke J, Raaphorst Joost, Löwenberg Mark, Takkenberg R Bart, D'Haens Geert R A M, Spuls Phyllis I, Bekkenk Marcel W, Musters Annelie H, Post Nicoline F, Bosma Angela L, Hilhorst Marc L, Vegting Yosta, Bemelman Frederike J, Voskuyl Alexandre E, Broens Bo, Parra Sanchez Agner, van Els Cécile A C M, de Wit Jelle, Rutgers Abraham, de Leeuw Karina, Horváth Barbara, Verschuuren Jan J G M, Ruiter Annabel M, van Ouwerkerk Lotte, van der Woude Diane, Allaart Cornelia F, Teng Y K Onno, van Paassen Pieter, Busch Matthias H, Jallah Papay B P, Brusse Esther, van Doorn Pieter A, Baars Adája E, Hijnen Dirk Jan, Schreurs Corine R G, van der Pol W Ludo, Goedee H Stephan, Vogelzang Erik H, Leeuw Maureen, Atiqi Sadaf, van Vollenhoven Ronald, Gerritsen Martijn, van der Horst-Bruinsma Irene E, Lems Willem F, Nurmohamed Mike T, Boers Maarten, Keijzer Sofie, Keijser Jim, van de Sandt Carolien, Boogaard Arend, Cristianawati Olvi, Ten Brinke Anja, Verstegen Niels J M, Zwinderman Koos A H, van Ham S Marieke, Rispens Theo, Kuijpers Taco W, Wolbink Gertjan, Eftimov Filip
Department of Rheumatology, Amsterdam Rheumatology and Immunology Center, location Reade, Amsterdam, Netherlands.
Department of Neurology and Neurophysiology, Amsterdam Neuroscience, University of Amsterdam, Amsterdam, Netherlands.
Lancet Rheumatol. 2022 Jun;4(6):e417-e429. doi: 10.1016/S2665-9913(22)00102-3. Epub 2022 Apr 29.
Concerns have been raised regarding the risks of SARS-CoV-2 breakthrough infections in vaccinated patients with immune-mediated inflammatory diseases treated with immunosuppressants, but clinical data on breakthrough infections are still scarce. The primary objective of this study was to compare the incidence and severity of SARS-CoV-2 breakthrough infections between patients with immune-mediated inflammatory diseases using immunosuppressants, and controls (patients with immune-mediated inflammatory diseases not taking immunosuppressants and healthy controls) who had received full COVID-19 vaccinations. The secondary objective was to explore determinants of breakthrough infections of the delta (B.1.617.2) variant of SARS-CoV-2, including humoral immune responses after vaccination.
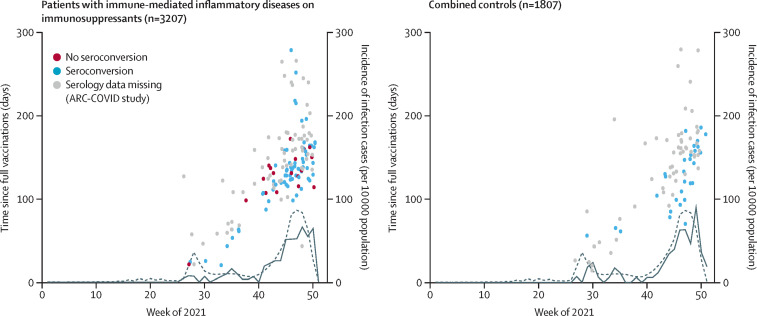
In this substudy, we pooled data collected in two large ongoing prospective multicentre cohort studies conducted in the Netherlands (Target to-B! [T2B!] study and Amsterdam Rheumatology Center COVID [ARC-COVID] study). Both studies recruited adult patients (age ≥18 years) with immune-mediated inflammatory diseases and healthy controls. We sourced clinical data from standardised electronic case record forms, digital questionnaires, and medical files. We only included individuals who were vaccinated against SARS-CoV-2. For T2B!, participants were recruited between Feb 2 and Aug 1, 2021, and for ARC-COVID, participants were recruited between April 26, 2020, and March 1, 2021. In this study we assessed data on breakthrough infections collected between July 1 and Dec 15, 2021, a period in which the delta SARS-CoV-2 variant was the dominant variant in the Netherlands. We defined a SARS-CoV-2 breakthrough infection as a PCR-confirmed or antigen test-confirmed SARS-CoV-2 infection that occurred at least 14 days after vaccination. All breakthrough infections during this period were assumed to be due to the delta variant due to its dominance during the study period. We analysed post-vaccination serum samples for anti-receptor binding domain (RBD) antibodies to assess the humoral vaccination response (T2B! study only) and anti-nucleocapsid antibodies to identify asymptomatic breakthrough infections (ARC-COVID study only). We used multivariable logistic regression analyses to explore potential clinical and humoral determinants associated with the odds of breakthrough infections. The T2B! study is registered with the Dutch Trial Register, Trial ID NL8900, and the ARC-COVID study is registered with Dutch Trial Register, trial ID NL8513.
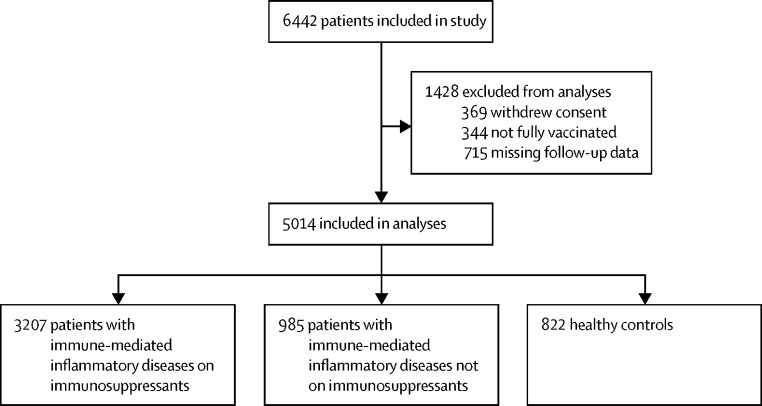
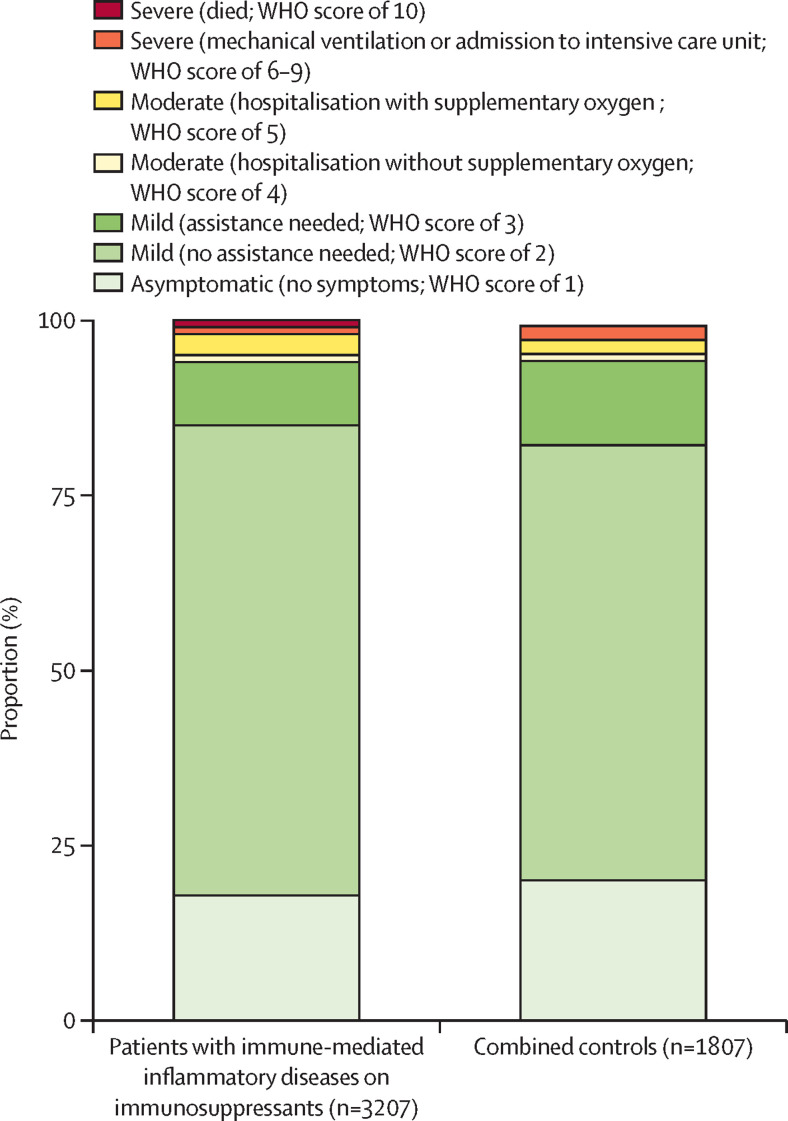
We included 3207 patients with immune-mediated inflammatory diseases who receive immunosuppressants, and 1807 controls (985 patients with immune-mediated inflammatory disease not on immunosuppressants and 822 healthy controls). Among patients receiving immunosuppressants, mean age was 53 years (SD 14), 2042 (64%) of 3207 were female and 1165 (36%) were male; among patients not receiving immunosuppressants, mean age was 54 years (SD 14), 598 (61%) of 985 were female and 387 (39%) were male; and among healthy controls, mean age was 57 years (SD 13), 549 (67%) of 822 were female and 273 (33%) were male. The cumulative incidence of PCR-test or antigen-test confirmed SARS-CoV-2 breakthrough infections was similar in patients on immunosuppressants (148 of 3207; 4·6% [95% CI 3·9-5·4]), patients not on immunosuppressants (52 of 985; 5·3% [95% CI 4·0-6·9]), and healthy controls (33 of 822; 4·0% [95% CI 2·8-5·6]). There was no difference in the odds of breakthrough infection for patients with immune-mediate inflammatory disease on immunosuppressants versus combined controls (ie, patients not on immunosuppressants and healthy controls; adjusted odds ratio 0·88 [95% CI 0·66-1·18]). Seroconversion after vaccination (odds ratio 0·58 [95% CI 0·34-0·98]; T2B! cohort only) and SARS-CoV-2 infection before vaccination (0·34 [0·18-0·56]) were associated with a lower odds of breakthrough infections.
The incidence and severity of SARS-CoV-2 breakthrough infections in patients with immune-mediated inflammatory diseases on immunosuppressants was similar to that in controls. However, caution might still be warranted for those on anti-CD20 therapy and those with traditional risk factors.
ZonMw (the Netherlands Organization for Health Research and Development) and Reade foundation.
对于接受免疫抑制剂治疗的免疫介导性炎症疾病疫苗接种患者出现新型冠状病毒2(SARS-CoV-2)突破性感染的风险,人们已有所担忧,但关于突破性感染的临床数据仍然匮乏。本研究的主要目的是比较使用免疫抑制剂的免疫介导性炎症疾病患者与接受全程2019冠状病毒病(COVID-19)疫苗接种的对照组(未服用免疫抑制剂的免疫介导性炎症疾病患者和健康对照)中SARS-CoV-2突破性感染的发生率和严重程度。次要目的是探讨SARS-CoV-2德尔塔(B.1.617.2)变异株突破性感染的决定因素,包括接种疫苗后的体液免疫反应。
在这项子研究中,我们汇总了在荷兰进行的两项正在进行的大型前瞻性多中心队列研究(目标到B![T2B!]研究和阿姆斯特丹风湿病中心COVID[ARC-COVID]研究)中收集的数据。两项研究均招募了患有免疫介导性炎症疾病的成年患者(年龄≥18岁)和健康对照。我们从标准化电子病例记录表格、数字问卷和医疗档案中获取临床数据。我们仅纳入了接种过SARS-CoV-2疫苗的个体。对于T2B!研究,参与者于2021年2月2日至8月1日招募;对于ARC-COVID研究,参与者于2020年4月26日至2021年3月1日招募。在本研究中,我们评估了2021年7月1日至12月15日期间收集的突破性感染数据,在此期间,SARS-CoV-2德尔塔变异株是荷兰的主要变异株。我们将SARS-CoV-2突破性感染定义为接种疫苗至少14天后经聚合酶链反应(PCR)确认或抗原检测确认的SARS-CoV-2感染。由于该变异株在研究期间占主导地位,因此假定在此期间所有突破性感染均由德尔塔变异株引起。我们分析了接种疫苗后的血清样本中的抗受体结合域(RBD)抗体以评估体液接种反应(仅T2B!研究)以及抗核衣壳抗体以识别无症状突破性感染(仅ARC-COVID研究)。我们使用多变量逻辑回归分析来探讨与突破性感染几率相关的潜在临床和体液决定因素。T2B!研究已在荷兰试验注册中心注册,试验编号NL8900,ARC-COVID研究已在荷兰试验注册中心注册,试验编号NL8513。
我们纳入了3207例接受免疫抑制剂治疗的免疫介导性炎症疾病患者和1807例对照(985例未服用免疫抑制剂的免疫介导性炎症疾病患者和822例健康对照)。在接受免疫抑制剂治疗的患者中,平均年龄为53岁(标准差14),3207例中有2042例(64%)为女性,1165例(36%)为男性;在未接受免疫抑制剂治疗的患者中,平均年龄为54岁(标准差14),985例中有598例(61%)为女性,387例(39%)为男性;在健康对照中,平均年龄为57岁(标准差13),822例中有549例(67%)为女性,273例(33%)为男性。接受免疫抑制剂治疗的患者、未接受免疫抑制剂治疗的患者和健康对照中,PCR检测或抗原检测确认的SARS-CoV-2突破性感染的累积发生率相似(3207例中的148例;4.6%[95%置信区间3.9 - 5.4])、未接受免疫抑制剂治疗的患者(985例中的52例;5.3%[95%置信区间4.0 - 6.9])和健康对照(822例中的33例;4.0%[95%置信区间2.8 - 5.6])。接受免疫抑制剂治疗的免疫介导性炎症疾病患者与联合对照组(即未接受免疫抑制剂治疗的患者和健康对照)相比,突破性感染的几率没有差异(调整后的优势比0.88[95%置信区间0.66 - 1.18])。接种疫苗后的血清转化(优势比0.58[95%置信区间0.34 - 0.98];仅T2B!队列)和接种疫苗前的SARS-CoV-2感染(0.34[0.18 - 0.56])与较低的突破性感染几率相关。
接受免疫抑制剂治疗的免疫介导性炎症疾病患者中SARS-CoV-2突破性感染的发生率和严重程度与对照组相似。然而,对于接受抗CD20治疗的患者和具有传统风险因素者,仍可能需要谨慎。
荷兰卫生研究与发展组织(ZonMw)和雷阿德基金会。