Simon David, Tascilar Koray, Fagni Filippo, Kleyer Arnd, Krönke Gerhard, Meder Christine, Dietrich Peter, Orlemann Till, Mößner Johanna, Taubmann Jule, Mutlu Melek Yalcin, Knitza Johannes, Kemenes Stephan, Liphardt Anna-Maria, Schönau Verena, Bohr Daniela, Schuster Louis, Hartmann Fabian, Minopoulou Ioanna, Leppkes Moritz, Ramming Andreas, Pachowsky Milena, Schuch Florian, Ronneberger Monika, Kleinert Stefan, Hueber Axel J, Manger Karin, Manger Bernhard, Atreya Raja, Berking Carola, Sticherling Michael, Neurath Markus F, Schett Georg
Department of Internal Medicine 3, Friedrich-Alexander University, Erlangen-Nuremberg and Universitätsklinikum Erlangen, Erlangen, Germany.
Deutsches Zentrum fuer Immuntherapie, Friedrich-Alexander University, Erlangen-Nuremberg and Universitätsklinikum Erlangen, Erlangen, Germany.
Lancet Rheumatol. 2022 Sep;4(9):e614-e625. doi: 10.1016/S2665-9913(22)00191-6. Epub 2022 Aug 9.
Concerns have been raised about the reduced immunogenicity of vaccines against SARS-CoV-2 in patients with immune-mediated inflammatory diseases and the higher risk of breakthrough infections. The objective of our study was to investigate the intensity and longevity of SARS-CoV-2 vaccination responses in patients with immune-mediated inflammatory diseases, and to assess the effects of diagnosis, treatment, and adapted vaccination schedules.
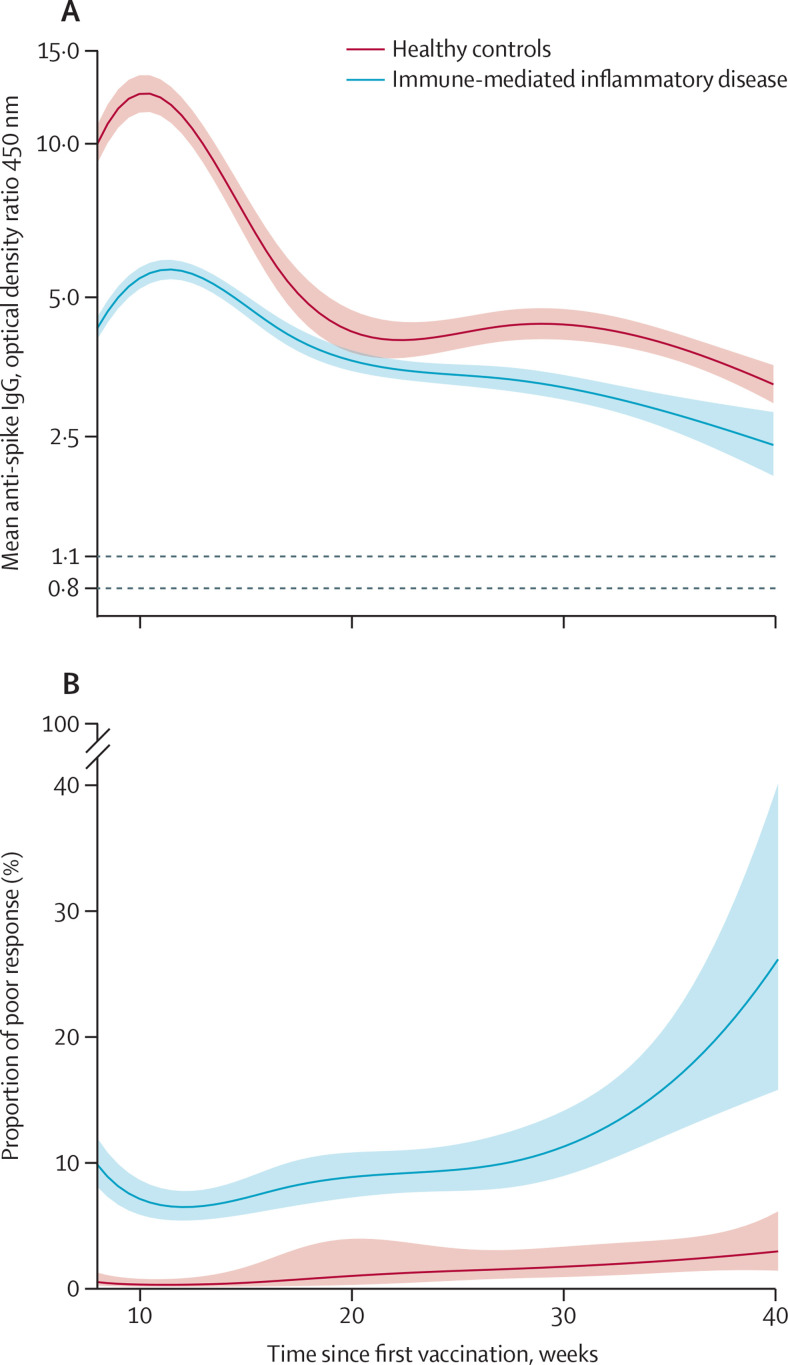
SARS-CoV-2 IgG antibody response after SARS-CoV-2 vaccination was measured over time in a large prospective cohort of healthy controls and participants with immune-mediated inflammatory diseases (attending or admitted to affiliated centres) between Dec 15, 2020, and Dec 1, 2021. Cohort participants with immune-mediated inflammatory diseases and control participants with no diagnosis of immune-mediated inflammatory diseases, were eligible for this analysis. Demographic data and disease-specific data were collected using a questionnaire. Humoral response was compared across treatment and disease groups, and with respect to the receipt of additional vaccinations. SARS-CoV-2 antibody response was measured by ELISA using optical density ratio units and modelled over time with age and sex adjustment using mixed-effects models. Using these models, marginal mean antibody titres and marginal risks of a poor response (optical density ratio <1·1) were calculated for each week starting from week 8 after the first vaccination to week 40.
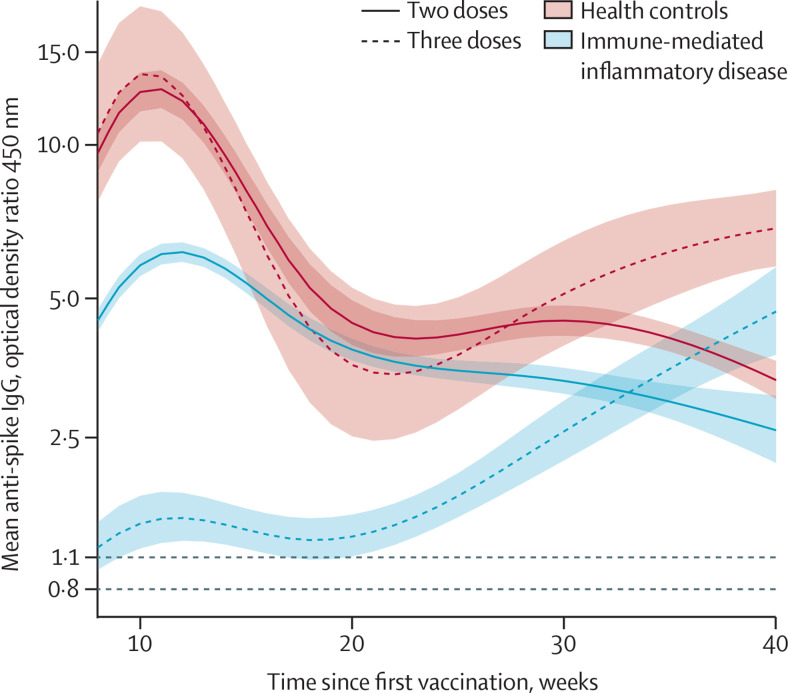
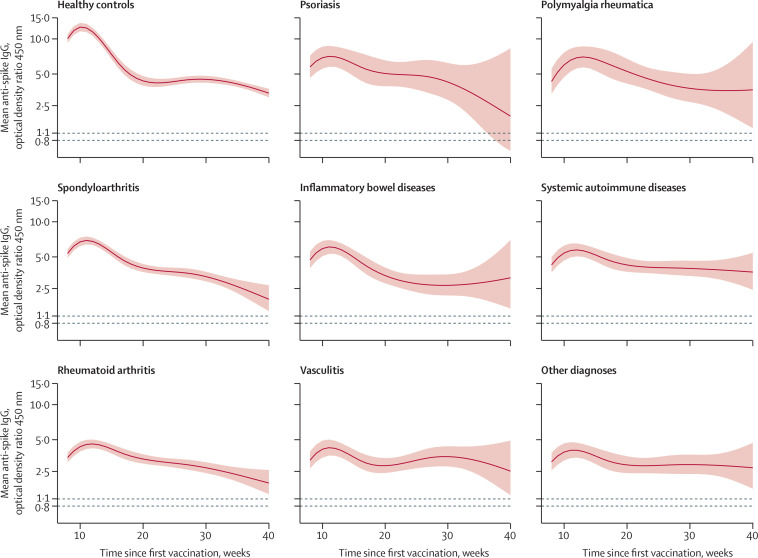
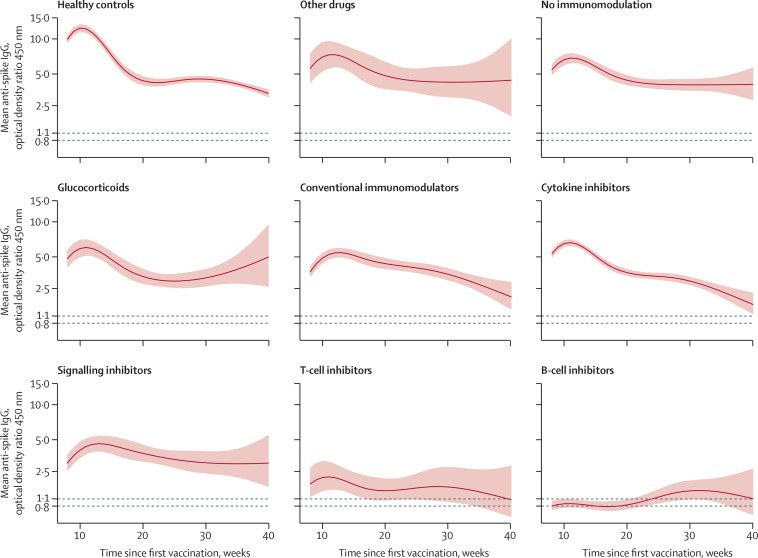
Among 5076 individuals registered, 2535 participants with immune-mediated inflammatory diseases (mean age 55·0 [15·2] years; 1494 [58·9%] women and 1041 [41·1%] men) and 1198 healthy controls (mean age 40·7 [13·5] years; 554 [46·2%] women and 644 [53·8%] men) were included in this analysis. Mean antibody titres were higher in healthy controls compared with people with immune-mediated inflammatory diseases at all timepoints, with a peak antibody response in healthy controls (mean optical density ratio 12·48; 95% CI 11·50-13·53) of more than twice that in participants with immune-mediated inflammatory diseases (5·50; 5·23-5·77; mean difference 6·98; 5·92-8·04). A poor response to vaccination was observed in participants with immune-mediated inflammatory diseases who were taking B-cell inhibitors (peak mean difference from healthy controls 11·68; 10·07-13·29) and T-cell inhibitors (peakmean difference from healthy controls 10·43; 8·33-12·53). Mean differences in antibody responses between different immune-mediated inflammatory diseases were small. Participants with immune-mediated inflammatory diseases who were given a third vaccine dose had higher mean antibody titres than did healthy controls vaccinated with two vaccine doses at 40 weeks after the initial vaccination (mean difference 1·34; 0·01-2·69).
People with immune-mediated inflammatory diseases show a lower and less durable SARS-CoV-2 vaccination response and are at risk of losing humoral immune protection. Adjusted vaccination schedules with earlier booster doses or more frequent re-doses, or both, could better protect people with immune-mediated inflammatory diseases.
Deutsche Forschungsgemeinschaft, Bundesministerium für Bildung und Forschung, European Research Council, Innovative Medicine Initiative, Friedrich-Alexander-Universität Erlangen-Nürnberg, Else Kröner-Memorial Foundation.
免疫介导的炎症性疾病患者中,针对严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗的免疫原性降低以及突破性感染风险较高,引发了人们的担忧。我们研究的目的是调查免疫介导的炎症性疾病患者中SARS-CoV-2疫苗接种反应的强度和持久性,并评估诊断、治疗及调整后的疫苗接种计划的效果。
在2020年12月15日至2021年12月1日期间,对一大组健康对照者和免疫介导的炎症性疾病参与者(在附属中心就诊或住院)进行前瞻性队列研究,随时间测量SARS-CoV-2疫苗接种后的SARS-CoV-2 IgG抗体反应。符合条件纳入本分析的队列参与者为患有免疫介导的炎症性疾病的患者以及未诊断为免疫介导的炎症性疾病的对照者。使用问卷收集人口统计学数据和疾病特异性数据。比较不同治疗组和疾病组之间以及接受额外疫苗接种者的体液反应。采用酶联免疫吸附测定法(ELISA)以光密度比值单位测量SARS-CoV-2抗体反应,并使用混合效应模型按年龄和性别调整后随时间进行建模。使用这些模型,计算从首次接种后第8周开始至第40周每周的边际平均抗体滴度和反应不佳(光密度比值<1.1)的边际风险。
在登记的5076人中,本分析纳入了2535名免疫介导的炎症性疾病参与者(平均年龄55.0[15.2]岁;1494名[58.9%]女性和1041名[41.1%]男性)和1198名健康对照者(平均年龄40.7[13.5]岁;554名[46.2%]女性和644名[53.8%]男性)。在所有时间点,健康对照者的平均抗体滴度均高于免疫介导的炎症性疾病患者,健康对照者的抗体反应峰值(平均光密度比值12.48;95%置信区间11.50 - 13.53)是免疫介导的炎症性疾病参与者(5.50;5.23 - 5.77;平均差异6.98;5.92 - 8.04)的两倍多。在服用B细胞抑制剂(与健康对照者的峰值平均差异11.68;10.07 - 13.29)和T细胞抑制剂(与健康对照者的峰值平均差异10.43;8.33 - 12.53)的免疫介导的炎症性疾病参与者中观察到疫苗接种反应不佳。不同免疫介导的炎症性疾病之间抗体反应的平均差异较小。在初次接种后40周,接受第三剂疫苗的免疫介导的炎症性疾病参与者的平均抗体滴度高于接种两剂疫苗的健康对照者(平均差异1.34;0.01 - 2.69)。
免疫介导的炎症性疾病患者的SARS-CoV-2疫苗接种反应较低且持续时间较短,存在失去体液免疫保护的风险。调整后的疫苗接种计划,如更早的加强剂量或更频繁的重复剂量,或两者兼用,可能会更好地保护免疫介导的炎症性疾病患者。
德国研究基金会、联邦教育与研究部、欧洲研究理事会、创新药物倡议、埃尔朗根 - 纽伦堡弗里德里希 - 亚历山大大学、埃尔丝·克罗纳纪念基金会。