Qu Shuping, Zhang Xiaobing, Wu Yutian, Meng Yan, Pan Hongyu, Fang Qiang, Hu Lei, Zhang Jin, Wang Ruoyu, Wei Lixin, Wu Dong
Department of Hepatic Surgery, Third Affiliated Hospital of Second Military Medical University, Shanghai, China.
Department of Hepatic Surgery, The First Hospital of Putian, Putian, China.
Front Oncol. 2022 Apr 21;12:874473. doi: 10.3389/fonc.2022.874473. eCollection 2022.
To compare the efficacy and safety of the combination of transcatheter arterial chemoembolization (TACE), Lenvatinib, and programmed cell death protein-1 (PD-1) inhibitors (combination group) with TACE (TACE group) in the treatment of patients with unresectable hepatocellular carcinoma (uHCC).
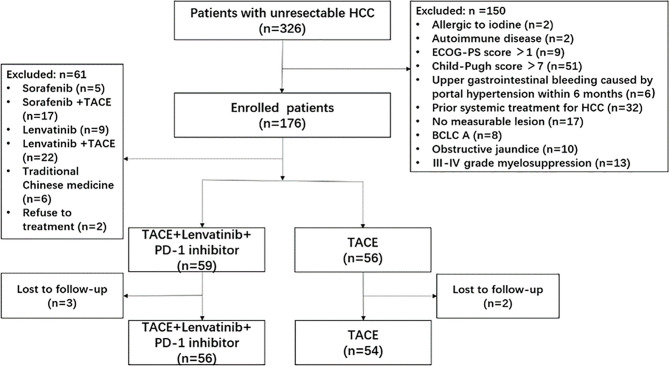
We consecutively enrolled 110 patients with uHCC in this prospective cohort study, with 56 patients receiving combination treatment and 54 patients receiving TACE from November 2017 to September 2020. The differences in tumor response, survival benefit, and adverse events (AEs) were compared between the two groups. Factors affecting survival were identified Cox regression analysis.
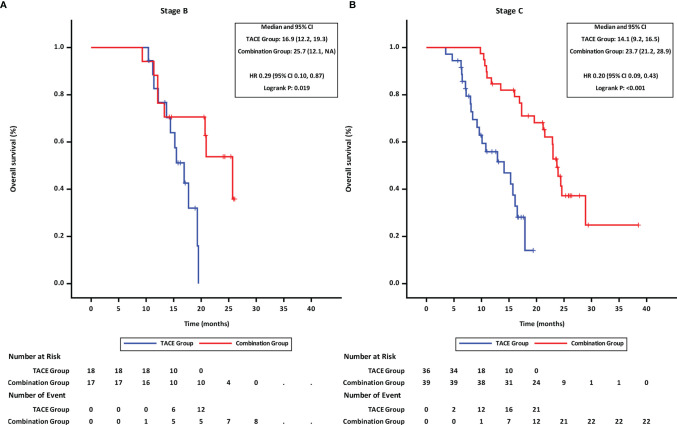
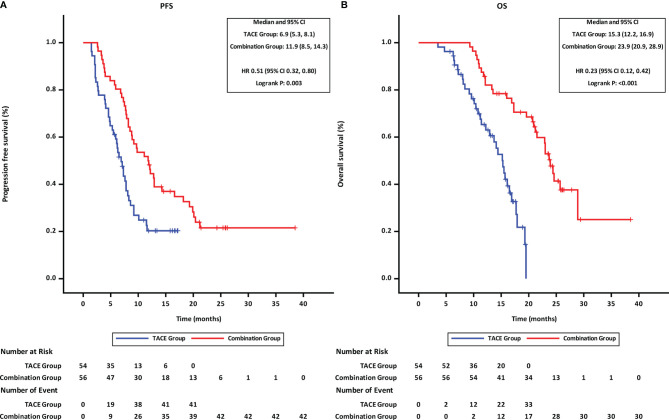
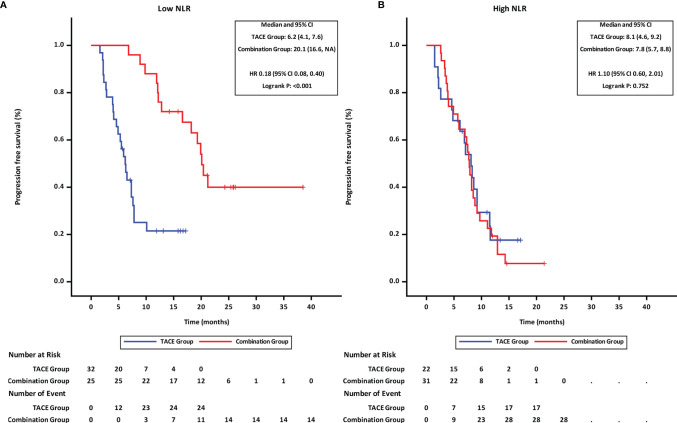
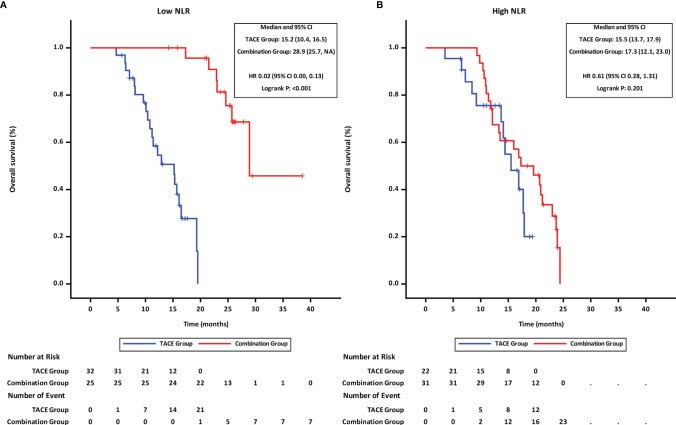
Compared with the TACE group, the combination group had a higher objective response rate (ORR) (67.9% vs. 29.6%, p < 0.001), longer median progression-free survival (mPFS) (11.9 vs. 6.9 months, P = 0.003) and overall survival (mOS) (23.9 vs. 15.3 months, p < 0.001). Multivariate analysis showed that the neutrophil-to-lymphocyte ratio (NLR) and the treatment option were independent factors associated with the PFS and OS. Further subgroup analysis showed that patients with low NLR (≤median 3.11) receiving combination therapy had better mPFS (20.1 vs. 6.2 months, P < 0.001) and mOS (28.9 vs. 15.2 months, P < 0.001) than those receiving TACE, while no obvious difference in PFS or OS was observed between the two groups in patients with high NLR (> 3.11). There were no unexpected toxicities in the combination group.
Compared with TACE, the combination treatment demonstrated an improved clinical efficacy and manageable safety profile in patients with uHCC. Combination treatment showed better therapeutic efficacy in patients with low NLR; therefore, this ratio could be used to identify patients who will benefit from this treatment.
比较经动脉化疗栓塞术(TACE)、乐伐替尼和程序性细胞死亡蛋白1(PD-1)抑制剂联合治疗(联合治疗组)与单纯TACE治疗(TACE组)对不可切除肝细胞癌(uHCC)患者的疗效和安全性。
在这项前瞻性队列研究中,我们连续纳入了110例uHCC患者,其中56例接受联合治疗,54例在2017年11月至2020年9月期间接受TACE治疗。比较两组患者的肿瘤反应、生存获益和不良事件(AE)差异。通过Cox回归分析确定影响生存的因素。
与TACE组相比,联合治疗组的客观缓解率(ORR)更高(67.9%对29.6%,p<0.001),中位无进展生存期(mPFS)更长(11.9个月对6.9个月,P=0.003),总生存期(mOS)更长(23.9个月对15.3个月,p<0.001)。多因素分析显示,中性粒细胞与淋巴细胞比值(NLR)和治疗方案是与PFS和OS相关的独立因素。进一步亚组分析显示,NLR低(≤中位数3.11)的联合治疗患者的mPFS(20.1个月对6.2个月,P<0.001)和mOS(28.9个月对15.2个月,P<0.001)优于接受TACE治疗的患者,而NLR高(>3.11)的患者两组之间在PFS或OS方面未观察到明显差异。联合治疗组未出现意外毒性。
与TACE相比,联合治疗在uHCC患者中显示出更好的临床疗效和可控的安全性。联合治疗在NLR低的患者中显示出更好的治疗效果;因此,该比值可用于识别将从该治疗中获益的患者。