Sun Wei, Luo Zujin, Cao Zhixin, Wang Jing, Zhang Liming, Ma Yingmin
Department of Respiratory and Critical Care Medicine, Beijing Chao-Yang Hospital, Capital Medical University, Beijing, China.
Department of Respiratory and Critical Care Medicine, Beijing Youan Hospital, Capital Medical University, Beijing, China.
Ann Transl Med. 2022 Apr;10(7):407. doi: 10.21037/atm-22-536.
Noninvasive ventilation (NIV) failure rate is relatively high in patients with acute respiratory distress syndrome (ARDS). Currently the data regarding prediction of NIV failure of pneumonia-induced mild to ARDS patients were scarce.
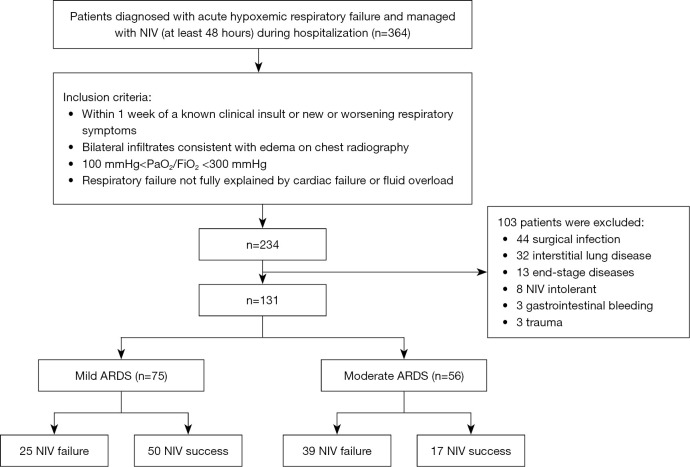
A total of 364 patients (from January 2016 to December 2020) diagnosed with hypoxemic respiratory failure and managed with NIV were initially included and finally 131 pneumonia-induced mild to moderate ARDS patients were enrolled in this study. Electronic medical records were reviewed to determine whether NIV succeeded or failed for each patient. The relationship between the Acute Physiology And Chronic Health Evaluation II (APACHE II) score , neutrophil/lymphocyte ratio (NLR), expired tidal volume (Vte) and NIV failure were specifically analyzed. Multivariate logistic regression analyses were conducted to identify the independent factors of NIV failure. Receiver-operating characteristic curves were used to assess the efficacy of the variables in predicting NIV failure. Kaplan-Meier curves for 28-day survival were used to compare the mortality rates of different groups.
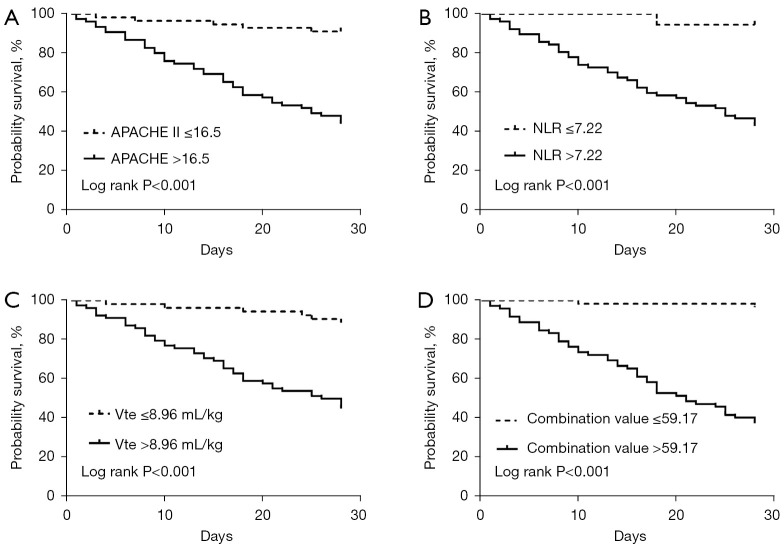
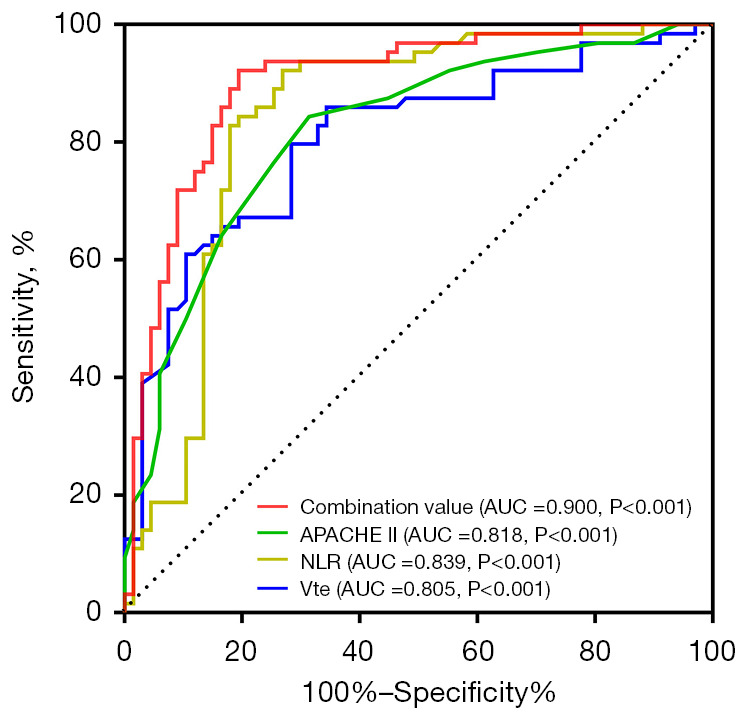
Of the patients, 64 (48.9%) experienced NIV failure, APACHE II score [odds ratio (OR) =0.77; P=0.002], NLR (OR =0.838; P=0.046), and Vte (OR =0.343; P=0.009) were independent factors for predicting NIV failure. A combined value comprising the APACHE II score, NLR, and Vte had better efficacy at predicting NIV failure [area under the curve (AUC) =0.9; 95% confidence interval (CI): 0.845-0.955] than the APACHE II score (AUC =0.818; 95% CI: 0.745-0.891), NLR (AUC =0.839; 95% CI: 0.765-0.913), or Vte (AUC =0.805; 95% CI: 0.729-0.881) alone. The cumulative survival probability within 28 days was lower in patients with a combined value >59.17 (P<0.001 by the log-rank test), an APACHE II score >16.5 (P<0.001 by the log-rank test), an NLR >7.22 (P<0.001 by the log-rank test), and a Vte >8.96 mL/kg (P<0.001 by log-rank test).
A combined value comprising an APACHE II score >16.5, a NLR >7.22, and a Vte >8.96 mL/kg may be a useful surrogate for predicting NIV failure among pneumonia-induced ARDS patients, and patients with a combined value >59.17 should be cautiously monitored during NIV. A further study with a larger sample size is warranted.
急性呼吸窘迫综合征(ARDS)患者无创通气(NIV)失败率相对较高。目前,关于肺炎所致轻度至ARDS患者NIV失败预测的数据较少。
最初纳入了2016年1月至2020年12月期间共364例诊断为低氧性呼吸衰竭并接受NIV治疗的患者,最终131例肺炎所致轻度至中度ARDS患者纳入本研究。回顾电子病历以确定每位患者NIV成功或失败。具体分析急性生理与慢性健康状况评分系统II(APACHE II)评分、中性粒细胞/淋巴细胞比值(NLR)、呼出潮气量(Vte)与NIV失败之间的关系。进行多因素逻辑回归分析以确定NIV失败的独立因素。采用受试者工作特征曲线评估各变量预测NIV失败的效能。使用28天生存的Kaplan-Meier曲线比较不同组的死亡率。
这些患者中,64例(48.9%)经历NIV失败,APACHE II评分[比值比(OR)=0.77;P=0.002]、NLR(OR =0.838;P=0.046)和Vte(OR =0.343;P=0.009)为预测NIV失败的独立因素。与单独的APACHE II评分(曲线下面积[AUC]=0.818;95%置信区间[CI]:0.745-0.891)、NLR(AUC =0.839;95% CI:0.765-0.913)或Vte(AUC =0.805;95% CI:0.729-0.881)相比,包含APACHE II评分、NLR和Vte的联合值在预测NIV失败方面具有更好的效能[AUC =0.9;95% CI:0.845-0.955]。联合值>59.17(对数秩检验P<0.001)、APACHE II评分>16.5(对数秩检验P<0.001)、NLR>7.22(对数秩检验P<0.001)和Vte>8.96 mL/kg(对数秩检验P<0.001)的患者28天内的累积生存概率较低。
APACHE II评分>16.5、NLR>7.22和Vte>8.96 mL/kg的联合值可能是预测肺炎所致ARDS患者NIV失败的有用替代指标,联合值>59.17的患者在NIV期间应谨慎监测。有必要进行更大样本量的进一步研究。