Department of Pathology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, No.17 Panjiayuan Nanli, Beijing, 100021, China.
Department of Medical Oncology, National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, China.
BMC Med. 2022 May 10;20(1):160. doi: 10.1186/s12916-022-02362-9.
Diverse genomic breakpoints of fusions that localize to intronic, exonic, or intergenic regions have been identified by DNA next-generation sequencing (NGS), but the role of exonic breakpoints remains elusive. We investigated whether exonic-breakpoint fusions could predict matched targeted therapy efficacy in non-small cell lung cancer (NSCLC).
NSCLC samples were analyzed by DNA NGS, RNA NGS, immunohistochemistry (IHC), and fluorescence in situ hybridization.
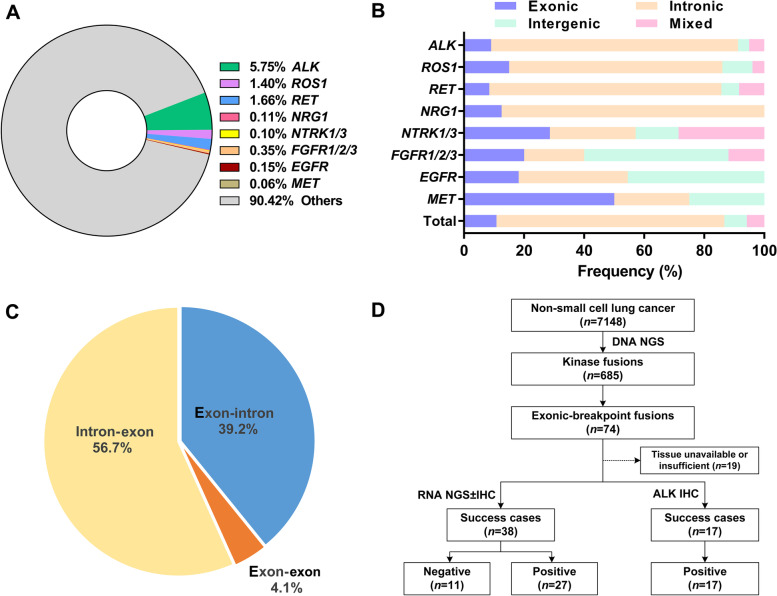
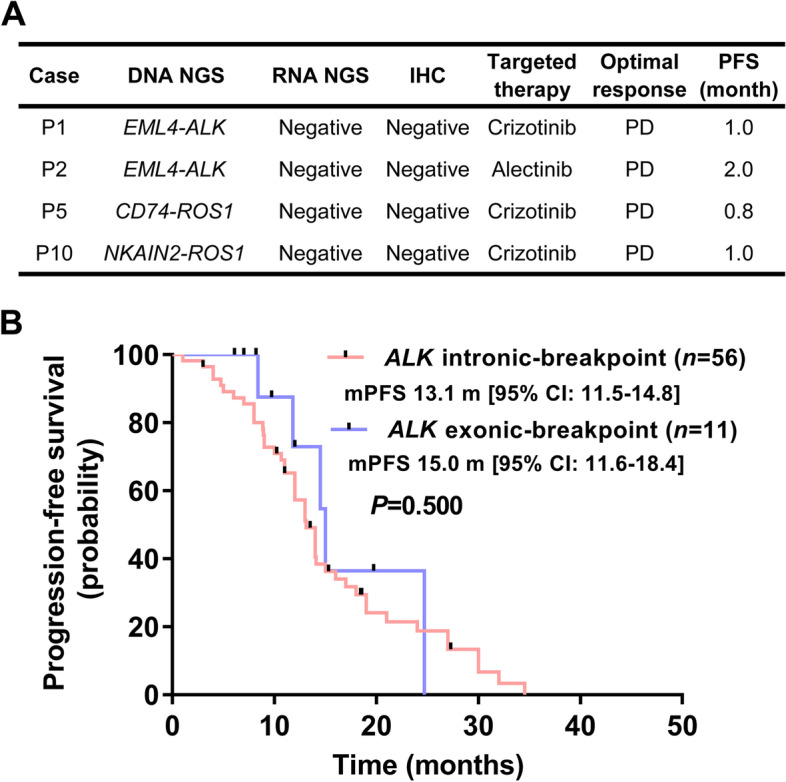
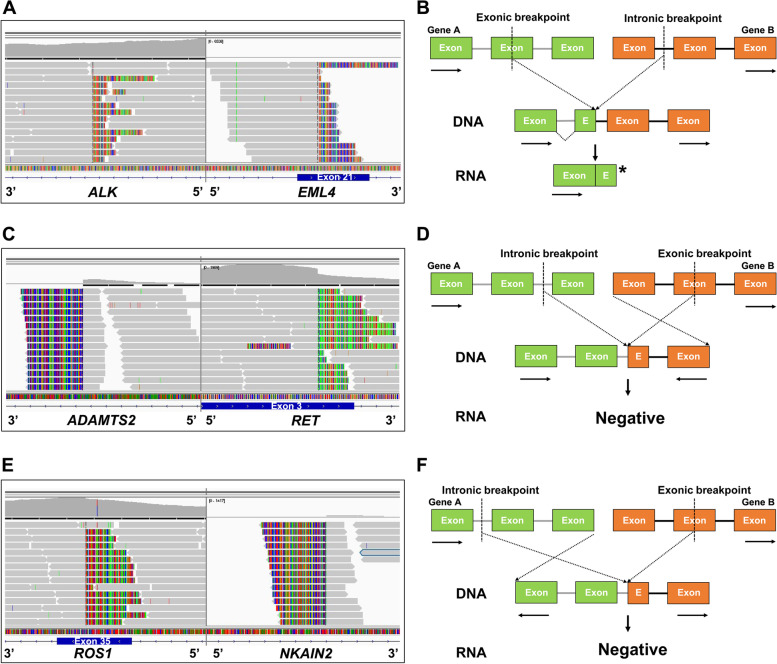
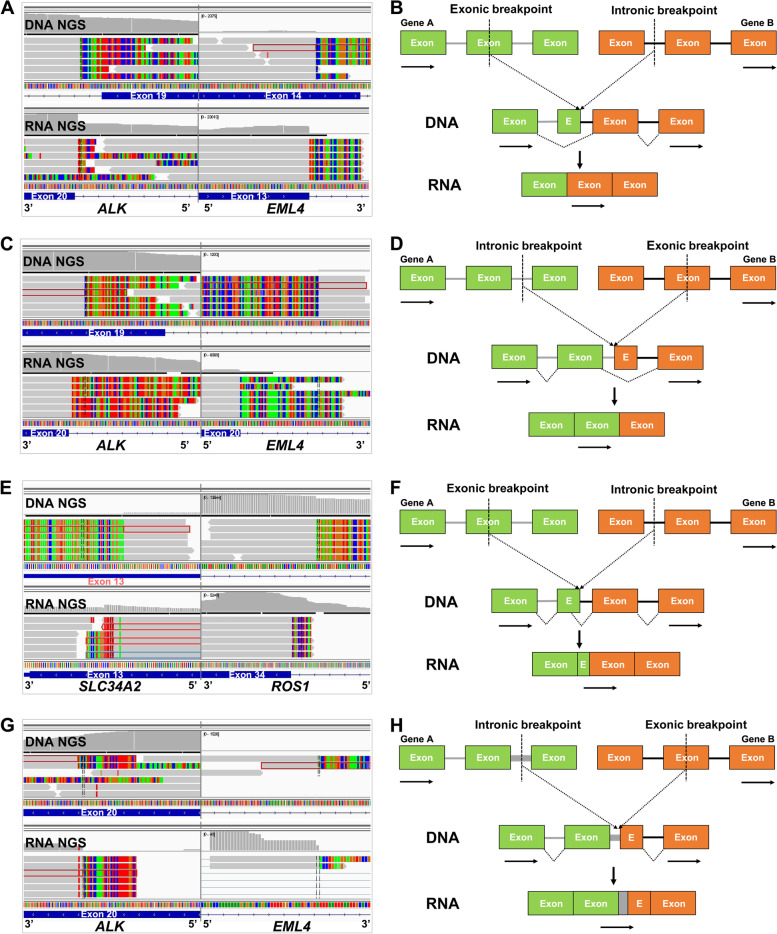
Using DNA NGS, kinase fusions were identified in 685 of 7148 (9.6%) NSCLCs, with 74 harboring exonic-breakpoint fusions, mostly anaplastic lymphoma kinase (ALK) fusions. RNA NGS and IHC revealed that 11 of 55 (20%) exonic-breakpoint fusions generated no aberrant transcript/protein, possibly due to open reading frame disruption or different gene transcriptional orientations. Four cases of genomic-positive but RNA/protein-negative fusions were treated with matched targeted therapy, but progressive disease developed within 2 months. Nevertheless, 44 of 55 (80%) exonic-breakpoint fusions produced chimeric transcripts/proteins, possibly owing to various alternative splicing patterns, including exon skipping, alternative splice site selection, and intron retention. Most of these genomic- and RNA/protein-positive fusion cases showed a clinical response to matched targeted therapy. Particularly, there were no differences in objective response rate (P = 0.714) or median progression-free survival (P = 0.500) between intronic-breakpoint (n = 56) and exonic-breakpoint ALK fusion subtypes (n = 11) among ALK RNA/protein-validated patients who received first-line crizotinib.
Exonic-breakpoint fusions may generate in-frame fusion transcripts/proteins or not, and thus are unreliable for predicting the efficacy of targeted therapy, which highlights the necessity of implementing RNA or protein assays for functional validation in exonic-breakpoint fusion cases.
通过 DNA 下一代测序(NGS)已经鉴定了定位于内含子、外显子或基因间区域的融合的不同基因组断点,但外显子断点的作用仍不清楚。我们研究了外显子断点融合是否可以预测非小细胞肺癌(NSCLC)中匹配的靶向治疗疗效。
通过 DNA NGS、RNA NGS、免疫组化(IHC)和荧光原位杂交分析 NSCLC 样本。
使用 DNA NGS,在 7148 例 NSCLC 中鉴定出 685 例激酶融合,其中 74 例存在外显子断点融合,主要是间变性淋巴瘤激酶(ALK)融合。RNA NGS 和 IHC 显示,55 例外显子断点融合中有 11 例未产生异常转录本/蛋白,可能是由于开放阅读框中断或不同基因转录方向。4 例基因组阳性但 RNA/蛋白阴性的融合接受了匹配的靶向治疗,但在 2 个月内疾病进展。然而,55 例外显子断点融合中有 44 例产生嵌合转录本/蛋白,可能是由于不同的选择性剪接模式,包括外显子跳跃、选择性剪接位点选择和内含子保留。这些基因组和 RNA/蛋白阳性融合病例中的大多数对匹配的靶向治疗有临床反应。特别是,在接受一线克唑替尼治疗的 ALK RNA/蛋白验证患者中,ALK 融合亚型中,外显子断点(n = 56)和外显子断点 ALK 融合亚型(n = 11)之间的客观缓解率(P = 0.714)或中位无进展生存期(P = 0.500)无差异。
外显子断点融合可能产生框架内融合转录本/蛋白,也可能不产生,因此不能可靠地预测靶向治疗的疗效,这突出了在外显子断点融合病例中进行 RNA 或蛋白检测进行功能验证的必要性。