Paediatric Haemato-oncology, Hospital Santa Casa de Belo Horizonte, Belo Horizonte, Brazil.
Instituto Nacional do Cancer, Research Center, Rio de Janeiro, Brazil.
JCO Glob Oncol. 2022 May;8:e2100425. doi: 10.1200/GO.21.00425.
International comparisons of patient demographics, tumor characteristics, and survival can shed light on areas for health care system improvement. The International Society of Pediatric Oncology Wilms Tumor 2001 trial/study registered patients through national clinical study groups in Western Europe and Brazil. This retrospective post hoc analysis of the International Society of Pediatric Oncology Wilms Tumor 2001 database aims to make visible and suggest reasons for any variations in outcomes.
All patients with unilateral Wilms tumor (WT), age > 6 months, treated with preoperative chemotherapy as per protocol, and registered between 2001 and 2011 were eligible. Countries were grouped to give comparable case numbers and geographical representation. Cox univariable and multivariable (MVA) statistics were applied, with the German collaborative group (Gesellschaft für Pädiatrische Onkologie und Hämatologie-Austria, Germany, and Switzerland) as reference for hazard ratios for event-free survival (EFS) and overall survival (OS).
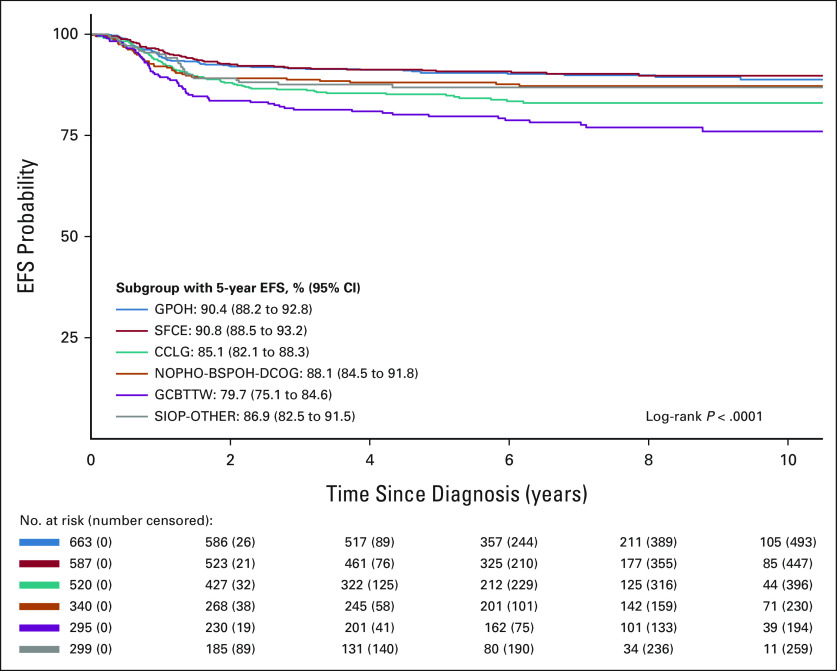
A total of 3,176 eligible patients were registered from 24 countries assigned into six groups. Age and histologic risk group distribution were similar across all groupings. The distribution of WT stage varied by country grouping, with 14.9% (range, 11.1%-18.2%) metastatic at diagnosis. Median follow-up was 78.9 months. For localized WT, 5-year EFS varied from 80% (Brazilian group) to 91% (French group; < .0001), retaining significance only for Brazil in MVA ( = .001). Five-year OS varied from 89% (Brazilian group) to 98% (French group; < .0001). In MVA, only superior OS in France was significant ( = .001). Five-year EFS/OS for stage IV did not vary significantly. High-risk histology and tumor volume at surgery were significantly associated with increased risk of death in MVA for metastatic disease.
International benchmarking of survival rates from WT within a large trial/study database has demonstrated statistically significant differences. Clinical interpretation should take account of variation in tumor stage but also treatment factors.
比较国际间患者人口统计学、肿瘤特征和生存情况,可以为改善医疗体系提供参考。国际儿科肿瘤协会威尔姆斯肿瘤 2001 试验/研究通过西欧和巴西的国家临床研究小组对患者进行登记。本研究对国际儿科肿瘤协会威尔姆斯肿瘤 2001 数据库进行回顾性事后分析,旨在发现并提出任何结果差异的原因。
所有符合单侧威尔姆斯肿瘤(WT)、年龄>6 个月、按照方案接受术前化疗、并于 2001 年至 2011 年期间登记的患者均符合条件。根据国家分组,使各组病例数和地理分布具有可比性。采用 Cox 单变量和多变量(MVA)统计方法,以德国协作组(德国、奥地利和瑞士的 Gesellschaft für Pädiatrische Onkologie und Hämatologie)为参考,计算无事件生存(EFS)和总生存(OS)的危险比。
共登记了 24 个国家的 3176 名符合条件的患者,分为 6 个组。所有组别的年龄和组织学危险分组分布相似。WT 分期的分布因国家分组而异,诊断时转移性肿瘤的比例为 14.9%(范围 11.1%~18.2%)。中位随访时间为 78.9 个月。对于局限性 WT,5 年 EFS 从巴西组的 80%到法国组的 91%( <.0001)不等,仅在 MVA 中巴西有显著差异( =.001)。5 年 OS 从巴西组的 89%到法国组的 98%( <.0001)不等。在 MVA 中,只有法国组的 OS 更高具有显著差异( =.001)。IV 期的 5 年 EFS/OS 无显著差异。高危组织学和手术时肿瘤体积在 MVA 中与转移性疾病死亡风险增加显著相关。
在大型试验/研究数据库中对 WT 生存率进行国际基准测试表明,存在统计学上的显著差异。临床解读应考虑肿瘤分期的差异,同时也应考虑治疗因素。