School of Biological Sciences, Monash University, Clayton, Victoria, Australia; Centre to Impact AMR, Monash University, Clayton, Victoria, Australia; Department of Infectious Diseases, The Alfred Hospital and Central Clinical School, Monash University, Melbourne, Victoria, Australia.
Centre to Impact AMR, Monash University, Clayton, Victoria, Australia; Infection Program, Department of Microbiology Monash University, Monash Biomedicine Discovery Institute, Clayton, Victoria, Australia.
EBioMedicine. 2022 Jun;80:104045. doi: 10.1016/j.ebiom.2022.104045. Epub 2022 May 7.
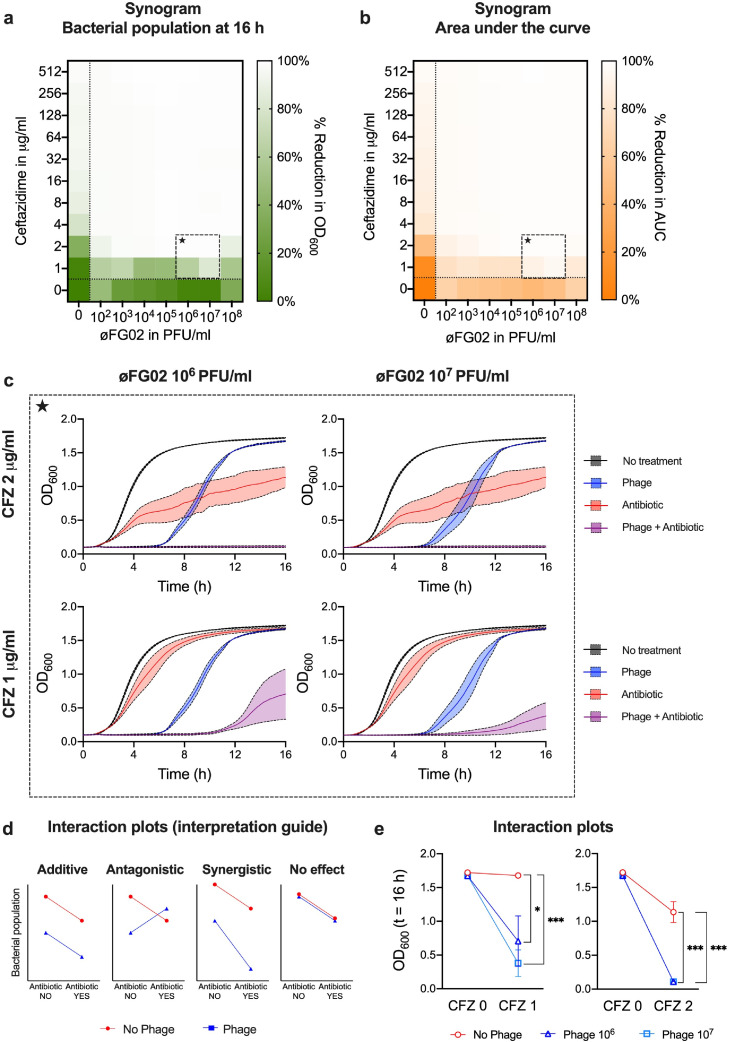
Clinical phage therapy is often delivered alongside antibiotics. However, the phenomenon of phage-antibiotic synergy has been mostly studied in vitro. Here, we assessed the in vivo bactericidal effect of a phage-antibiotic combination on Acinetobacter baumannii AB900 using phage øFG02, which binds to capsular polysaccharides and leads to antimicrobial resensitisation in vitro.
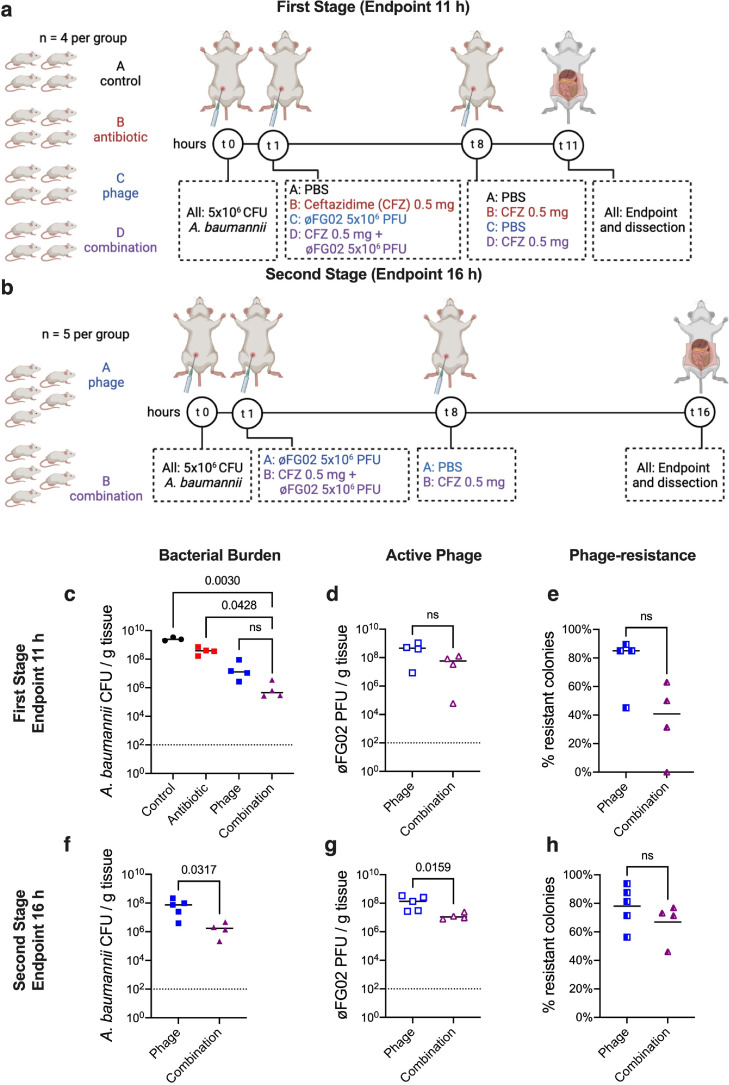
We performed a two-stage preclinical study using a murine model of severe A. baumannii AB900 bacteraemia. In the first stage, with an endpoint of 11 h, mice (n = 4 per group) were treated with either PBS, ceftazidime, phage øFG02, or the combination of phage and ceftazidime. The second stage involved only the latter two groups (n = 5 per group), with a prolonged endpoint of 16 h. The primary outcome was the average bacterial burden from four body sites (blood, liver, kidney, and spleen). Bacterial colonies from phage-treated mice were retrieved and screened for phage-resistance.
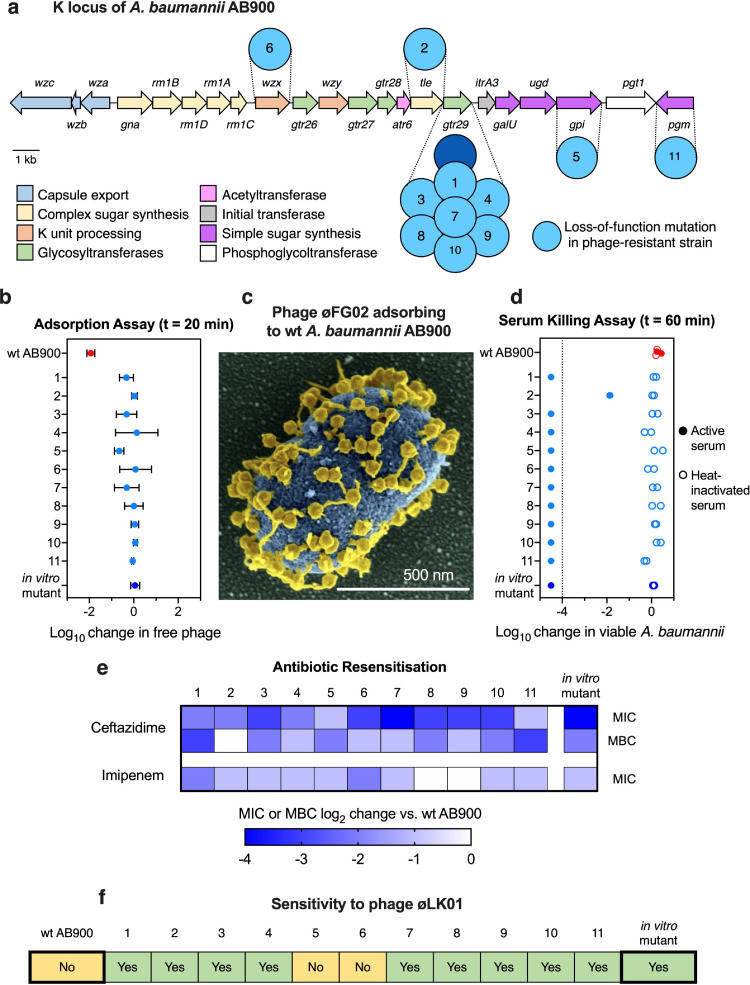
In the first stage, the bacterial burden (CFU/g of tissue) of the combination group (median: 4.55 × 10; interquartile range [IQR]: 2.79 × 10-2.81 × 10) was significantly lower than the PBS (median: 2.42 × 10; IQR: 1.97 × 10-3.48 × 10) and ceftazidime groups (median: 3.86 × 10; IQR: 2.15 × 10-6.35 × 10), but not the phage-only group (median: 1.28 × 10; IQR: 4.71 × 10-7.13 × 10). In the second stage, the combination treatment (median: 1.72 × 10; IQR: 5.11 × 10-4.00 × 10) outperformed the phage-only treatment (median: 7.46 × 10; IQR: 1.43 × 10-1.57 × 10). Phage-resistance emerged in 96% of animals receiving phages, and all the tested isolates (n = 11) had loss-of-function mutations in genes involved in capsule biosynthesis and increased sensitivity to ceftazidime.
øFG02 reliably drives the in vivo evolution of A. baumannii AB900 towards a capsule-deficient, phage-resistant phenotype that is resensitised to ceftazidime. This mechanism highlights the clinical potential of using phage therapy to target A. baumannii and restore antibiotic activity.
National Health and Medical Research Council (Australia).
临床噬菌体疗法通常与抗生素联合使用。然而,噬菌体-抗生素协同作用的现象主要在体外进行研究。在这里,我们使用噬菌体 øFG02 评估了噬菌体-抗生素联合对鲍曼不动杆菌 AB900 的体内杀菌作用,噬菌体 øFG02 结合荚膜多糖,导致体外抗菌敏化。
我们使用严重鲍曼不动杆菌 AB900 菌血症的小鼠模型进行了两阶段临床前研究。在第一阶段,以 11 小时为终点,每组(每组 4 只)用 PBS、头孢他啶、噬菌体 øFG02 或噬菌体和头孢他啶的联合治疗。第二阶段仅涉及后两组(每组 5 只),延长终点为 16 小时。主要结果是来自四个身体部位(血液、肝脏、肾脏和脾脏)的平均细菌负担。从噬菌体处理的小鼠中回收细菌菌落,并筛选噬菌体耐药性。
在第一阶段,联合组(中位数:4.55×10;四分位距 [IQR]:2.79×10-2.81×10)的细菌负荷(组织 CFU/g)明显低于 PBS 组(中位数:2.42×10;IQR:1.97×10-3.48×10)和头孢他啶组(中位数:3.86×10;IQR:2.15×10-6.35×10),但不低于噬菌体单一组(中位数:1.28×10;IQR:4.71×10-7.13×10)。在第二阶段,联合治疗(中位数:1.72×10;IQR:5.11×10-4.00×10)优于噬菌体单一组(中位数:7.46×10;IQR:1.43×10-1.57×10)。接受噬菌体治疗的动物中有 96%出现噬菌体耐药性,所有测试分离株(n=11)在参与荚膜生物合成的基因中均存在功能丧失突变,并且对头孢他啶的敏感性增加。
øFG02 可靠地驱动鲍曼不动杆菌 AB900 在体内向荚膜缺陷、噬菌体耐药表型进化,并恢复对头孢他啶的敏感性。这种机制突出了噬菌体治疗靶向鲍曼不动杆菌并恢复抗生素活性的临床潜力。
澳大利亚国家卫生和医学研究委员会。