Department of Cardiology, Copenhagen University Hospital - Bispebjerg and Frederiksberg, Copenhagen, Denmark.
Department of Cardiology, Copenhagen University Hospital - Herlev and Gentofte, Copenhagen, Denmark.
Cardiology. 2022;147(3):235-247. doi: 10.1159/000524948. Epub 2022 May 10.
Unstable angina (UA) is a component of acute coronary syndrome that is only occasionally included in primary composite endpoints in clinical cardiovascular trials. The aim of this paper is to elucidate the potential benefits and disadvantages of including UA in such contexts.
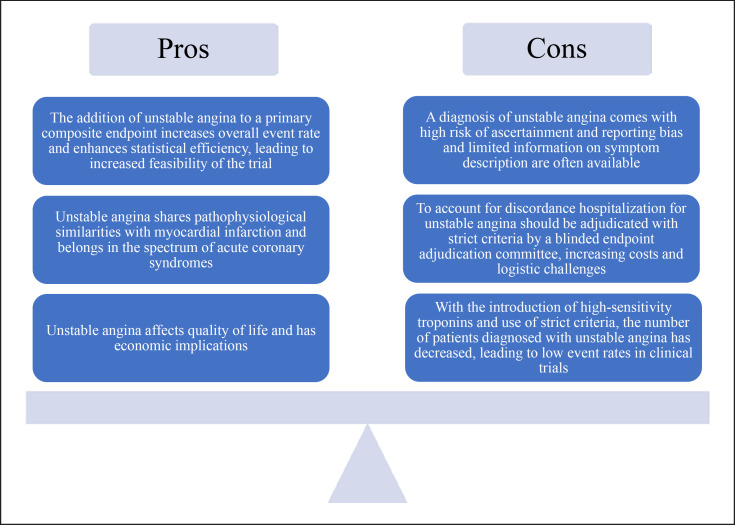
UA comprises <10% of patients with acute coronary syndromes in contemporary settings. Based on the pathophysiological similarities, it is ideal as a part of a composite endpoint along with myocardial infarction (MI). By adding UA as a component of a primary composite endpoint, the number of events and feasibility of the trial should increase, thus decreasing its size and cost. Furthermore, UA has both economic and quality of life implications on a societal and an individual level. However, there are important challenges associated with the use of UA as an endpoint. With the introduction of high-sensitivity troponins, the number of individuals diagnosed with UA has decreased to rather low levels, with a reciprocal increase in the number of MI. In addition, UA is particularly challenging to define given the subjective assessment of the index symptoms, rendering a high risk of bias. To minimize bias, strict criteria are warranted, and events should be adjudicated by a blinded endpoint adjudication committee.
UA should only be chosen as a component of a primary composite endpoint in cardiovascular trials after thoroughly evaluating the pros and cons. If it is chosen to include UA, appropriate precautions should be taken to minimize possible bias.
不稳定型心绞痛(UA)是急性冠状动脉综合征的一个组成部分,在临床心血管试验中仅偶尔包含在主要复合终点中。本文的目的是阐明在这种情况下纳入 UA 的潜在益处和弊端。
在当代情况下,UA 占急性冠状动脉综合征患者的<10%。基于病理生理学上的相似性,它是与心肌梗死(MI)一起作为复合终点的理想组成部分。通过将 UA 作为主要复合终点的一部分纳入,事件的数量和试验的可行性应该会增加,从而降低其规模和成本。此外,UA 在社会和个人层面上都对经济和生活质量产生影响。
然而,将 UA 用作终点存在重要挑战。随着高敏肌钙蛋白的引入,被诊断为 UA 的人数已降至相当低的水平,而 MI 的人数则相应增加。此外,UA 特别难以定义,因为需要对指数症状进行主观评估,从而存在很高的偏倚风险。为了最大程度地减少偏倚,需要严格的标准,并且应该由盲法终点裁决委员会来裁决事件。
只有在彻底评估利弊后,UA 才应作为心血管试验主要复合终点的组成部分。如果选择包含 UA,则应采取适当的预防措施以最大程度地减少可能的偏倚。