Bosco Elliott, Hsueh Leon, McConeghy Kevin W, Gravenstein Stefan, Saade Elie
Department of Health Services, Policy, and Practice, Brown University School of Public Health, 121 South Main Street, Box G-S121-3, Providence, RI, 02912, USA.
Center for Gerontology and Healthcare Research, Brown University School of Public Health, RI, Providence, USA.
BMC Med Res Methodol. 2021 Nov 6;21(1):241. doi: 10.1186/s12874-021-01440-5.
Major adverse cardiovascular events (MACE) are increasingly used as composite outcomes in randomized controlled trials (RCTs) and observational studies. However, it is unclear how observational studies most commonly define MACE in the literature when using administrative data.
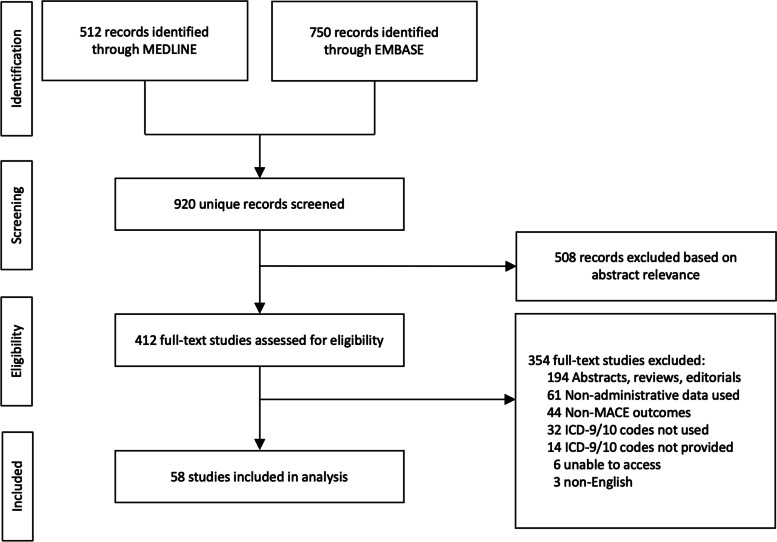
We identified peer-reviewed articles published in MEDLINE and EMBASE between January 1, 2010 to October 9, 2020. Studies utilizing administrative data to assess the MACE composite outcome using International Classification of Diseases 9th or 10th Revision diagnosis codes were included. Reviews, abstracts, and studies not providing outcome code definitions were excluded. Data extracted included data source, timeframe, MACE components, code definitions, code positions, and outcome validation.
A total of 920 articles were screened, 412 were retained for full-text review, and 58 were included. Only 8.6% (n = 5/58) matched the traditional three-point MACE RCT definition of acute myocardial infarction (AMI), stroke, or cardiovascular death. None matched four-point (+unstable angina) or five-point MACE (+unstable angina and heart failure). The most common MACE components were: AMI and stroke, 15.5% (n = 9/58); AMI, stroke, and all-cause death, 13.8% (n = 8/58); and AMI, stroke and cardiovascular death 8.6% (n = 5/58). Further, 67% (n = 39/58) did not validate outcomes or cite validation studies. Additionally, 70.7% (n = 41/58) did not report code positions of endpoints, 20.7% (n = 12/58) used the primary position, and 8.6% (n = 5/58) used any position.
Components of MACE endpoints and diagnostic codes used varied widely across observational studies. Variability in the MACE definitions used and information reported across observational studies prohibit the comparison, replication, and aggregation of findings. Studies should transparently report the administrative codes used and code positions, as well as utilize validated outcome definitions when possible.
主要心血管不良事件(MACE)越来越多地被用作随机对照试验(RCT)和观察性研究中的复合结局。然而,目前尚不清楚在使用管理数据时,观察性研究在文献中最常如何定义MACE。
我们检索了2010年1月1日至2020年10月9日期间发表在MEDLINE和EMBASE上的同行评审文章。纳入使用管理数据并利用国际疾病分类第9版或第10版诊断编码评估MACE复合结局的研究。排除综述、摘要以及未提供结局编码定义的研究。提取的数据包括数据源、时间范围、MACE组成部分、编码定义、编码位置和结局验证。
共筛选出920篇文章,412篇保留进行全文评审,58篇被纳入。只有8.6%(n = 5/58)符合急性心肌梗死(AMI)、中风或心血管死亡的传统三点MACE RCT定义。没有一项符合四点(+不稳定型心绞痛)或五点MACE(+不稳定型心绞痛和心力衰竭)。最常见的MACE组成部分是:AMI和中风,15.5%(n = 9/58);AMI、中风和全因死亡,13.8%(n = 8/58);以及AMI、中风和心血管死亡,8.6%(n = 5/58)。此外,67%(n = 39/58)未对结局进行验证或引用验证研究。另外,70.7%(n = 41/58)未报告终点的编码位置,20.7%(n = 12/58)使用主要位置,8.6%(n = 5/58)使用任何位置。
观察性研究中使用的MACE终点组成部分和诊断编码差异很大。观察性研究中使用的MACE定义和报告信息的变异性阻碍了研究结果的比较、重复和汇总。研究应透明地报告所使用的管理编码和编码位置,并尽可能使用经过验证的结局定义。