School of Basic Medical Sciences, Yunnan University of Chinese Medicine, Kunming, China.
The First School of Clinical Medicine, Yunnan University of Chinese Medicine, Kunming, China.
Front Public Health. 2022 Apr 25;10:875558. doi: 10.3389/fpubh.2022.875558. eCollection 2022.
Attenuated humoral response to mRNA SARS-CoV-2 vaccines has been reported in some patients with autoimmune disease, e.g., rheumatoid arthritis (RA). However, data of immune responses to inactivated SARS-CoV-2 vaccine in the RA population are still unknown. Herein, the safety and immunogenicity of inactivated SARS-CoV-2 vaccines in RA patients were analyzed.
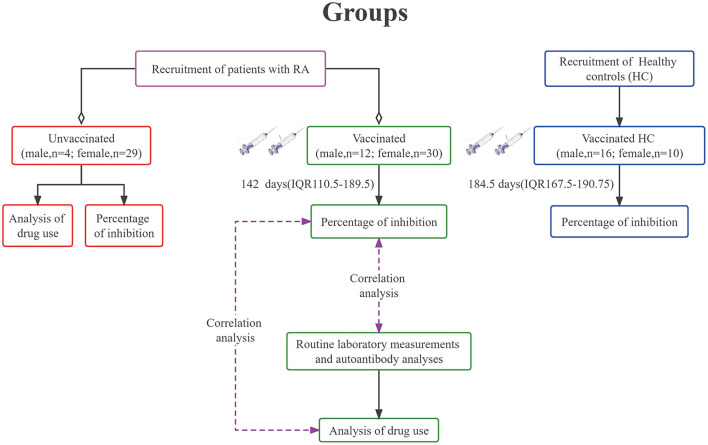
Seventy five RA patients and 26 healthy controls (HC) were respectively recruited from Yunnan Provincial Hospital of Traditional Chinese Medicine and the community in Kunming city. Neutralizing Antibody (NAb) Test ELISA kit was used to measure the percentage of inhibition. AKA (anti-keratin antibody) positivity was detected using indirect immunofluorescence. Rheumatoid factor (RF)-IgA was detected by ELISA. RF-IgG, RF-IgM, and anti-cyclic citrullinated peptide (CCP) antibodies were measured by chemiluminescence. ESR (erythrocyte sedimentation rate) was detected by ESR analyzer. C-RP (c-reactive protein) was detected by immunoturbidimetry. NEUT% (percentage of neutrophils) and LYMPH% (percentage of percentage) were calculated by a calculation method.
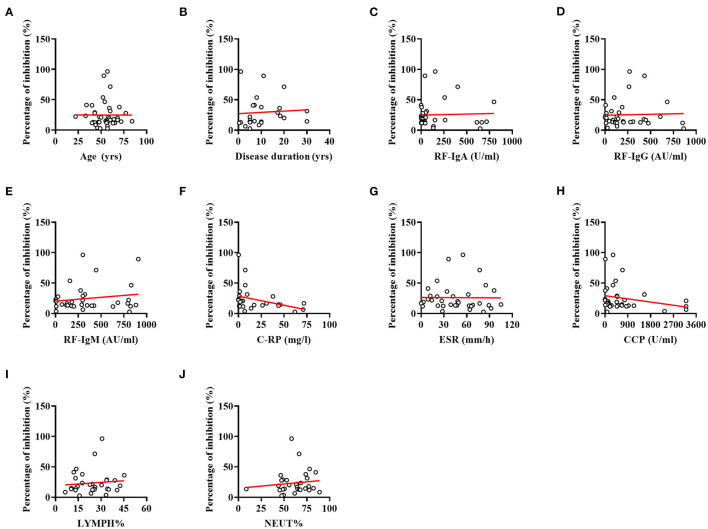
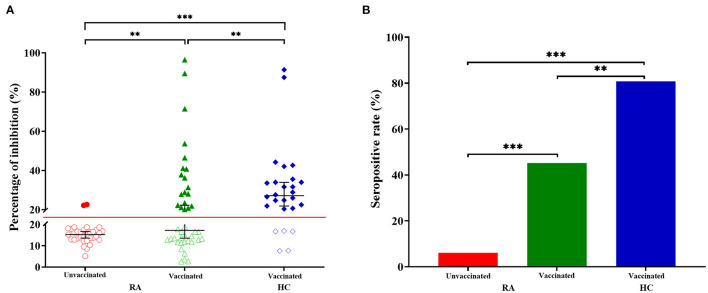
Compared with the HC group, the percentage of inhibition was significantly lower in RA patients receiving two doses of vaccines. Vaccines-induced percentage of inhibition was the lowest in RA patients who had not been vaccinated. In total 80.77% of the HC group had a percentage of inhibition ≧20%, compared with 45.24% of vaccinated RA patients and 6.06% of unvaccinated RA patients. Spearman correlation analysis revealed that antibody responses to SARS-CoV-2 did not differ between RA patients according to their age and disease duration. Furthermore, the results showed that no correlation was found between the percentage of inhibition and indices for RA, including RF-IgA, IgG, IgM; anti-CCP antibody; ESR; C-RP; NEUT% and LYMPH%.
Our study showed inactivated vaccine-induced SARS-COV-2 antibody responses differ in RA patients and healthy subjects, emphasizing the importance of a third or fourth vaccination in RA patients.
已报道某些自身免疫性疾病患者(例如类风湿关节炎)对 mRNA SARS-CoV-2 疫苗的体液免疫应答减弱。然而,关于 SARS-CoV-2 灭活疫苗在 RA 人群中的免疫反应的数据仍未知。在此,分析了 SARS-CoV-2 灭活疫苗在 RA 患者中的安全性和免疫原性。
分别从云南省中医院和昆明市社区招募了 75 名 RA 患者和 26 名健康对照者(HC)。使用中和抗体(NAb)检测 ELISA 试剂盒测量抑制百分比。使用间接免疫荧光法检测 AKA(抗角蛋白抗体)阳性。使用 ELISA 检测 RF-IgA。使用化学发光法测量 RF-IgG、RF-IgM 和抗环瓜氨酸肽(CCP)抗体。使用 ESR 分析仪检测 ESR(红细胞沉降率)。使用免疫比浊法检测 C-RP(c 反应蛋白)。通过计算法计算 NEUT%(中性粒细胞百分比)和 LYMPH%(淋巴细胞百分比)。
与 HC 组相比,接受两剂疫苗的 RA 患者的抑制百分比明显较低。未接种疫苗的 RA 患者的疫苗诱导抑制百分比最低。HC 组总共有 80.77%的患者抑制百分比≥20%,而接种疫苗的 RA 患者为 45.24%,未接种疫苗的 RA 患者为 6.06%。Spearman 相关性分析表明,根据年龄和疾病持续时间,RA 患者对 SARS-CoV-2 的抗体反应没有差异。此外,结果表明,抑制百分比与 RA 的各项指标(包括 RF-IgA、IgG、IgM;抗 CCP 抗体;ESR;C-RP;NEUT%和 LYMPH%)之间无相关性。
我们的研究表明,RA 患者和健康受试者对灭活疫苗诱导的 SARS-COV-2 抗体反应不同,强调了 RA 患者接种第三或第四剂疫苗的重要性。