Li Le, Zhang Zhenhao, Xiong Yulong, Hu Zhao, Liu Shangyu, Tu Bin, Yao Yan
National Center for Cardiovascular Diseases, Fu Wai Hospital, Peking Union Medical College, Chinese Academy of Medical Sciences, Beijing, China.
Front Cardiovasc Med. 2022 Apr 25;9:853217. doi: 10.3389/fcvm.2022.853217. eCollection 2022.
Decreased urine output (UO) is associated with adverse outcomes in certain patients, but this effect in patients admitted for cardiovascular diseases is still unproven. Moreover, the relationship between increased UO and prognosis is also unclear.
To investigate the relationship between decreased or increased UO and outcomes in patients with the cardiovascular intensive care unit (CICU).
This study was a retrospective cohort analysis based on the medical information mart for intensive care III (MIMIC-III) database. The patients' data were extracted from the Beth Israel Deaconess Medical Center (Boston, MA) between 2001 and 2012. With the initial 24-h UO range from 0.5 to 1.0 ml/kg/h as the reference, participants were divided into the several groups. The primary outcome was 30-day mortality. The secondary outcomes were 90-day mortality, ICU mortality, hospital mortality, use of mechanical ventilation (MV), and vasopressor agents in the first 24-h of ICU. The association between UO and mortality was assessed by multivariable logistic regression.
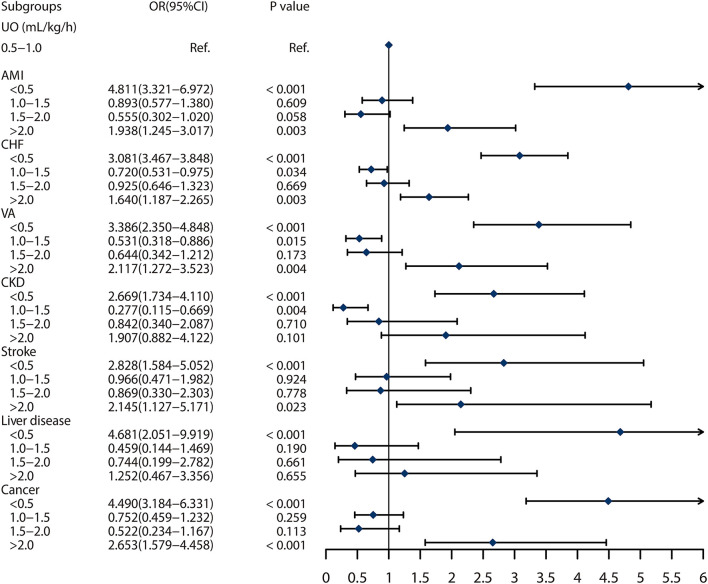
A total of 13,279 patients admitted to CICU were included. Low UO (< 0.5 ml/kg/h) was strongly associated with 30-day mortality (unadjusted OR = 3.993, 95% CI: 3.447-4.625, < 0.001), and very high UO (≥ 2.0 ml/kg/h) was also a significantly risk factor for 30-day mortality (Unadjusted OR = 2.069, 95% CI: 1.701-2.516, < 0.001) compared with the reference. The same effects also were shown in the multivariable logistic regression, adjusted by age, gender, vital signs, common comorbidities, and use of diuretics, with an adjusted OR of 2.023 (95% CI: 1.693-2.417, < 0.001) for low UO and 1.771 (95% CI: 1.389-2.256, < 0.001) for very high UO. Moreover, both decreased UO and increased UO were risk factors for 90-day mortality, ICU mortality, hospital mortality, use of MV and vasopressor agents.
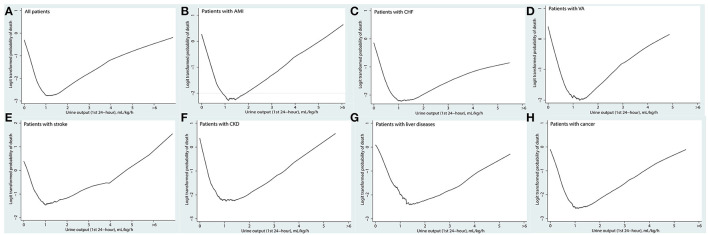
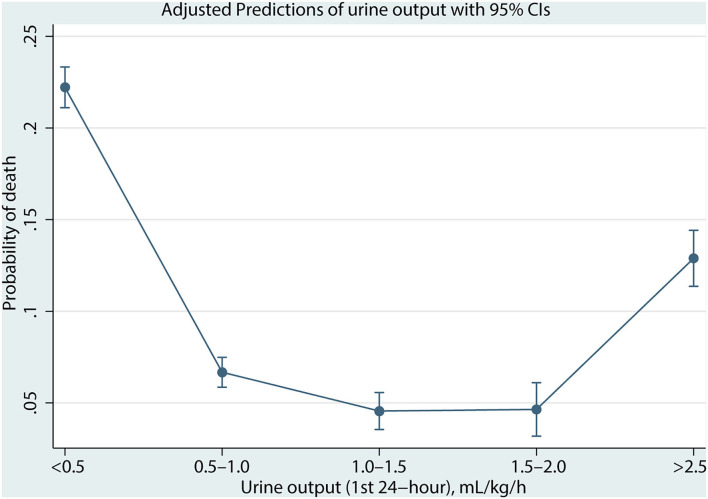
The decreased and increased UO both were significantly associated with short-term mortality, the relationship between UO and mortality was U-shape rather than linear.
尿量减少(UO)与某些患者的不良结局相关,但在因心血管疾病入院的患者中,这种影响仍未得到证实。此外,尿量增加与预后之间的关系也不清楚。
探讨心血管重症监护病房(CICU)患者尿量减少或增加与预后的关系。
本研究是基于重症监护医学信息集市III(MIMIC-III)数据库的回顾性队列分析。患者数据来自2001年至2012年期间的贝斯以色列女执事医疗中心(马萨诸塞州波士顿)。以初始24小时尿量范围为0.5至1.0 ml/kg/h作为参考,将参与者分为几组。主要结局是30天死亡率。次要结局是90天死亡率、ICU死亡率、医院死亡率、机械通气(MV)的使用以及ICU前24小时内血管升压药的使用。通过多变量逻辑回归评估尿量与死亡率之间的关联。
共纳入13279例入住CICU的患者。低尿量(<0.5 ml/kg/h)与30天死亡率密切相关(未调整的OR = 3.993,95%CI:3.447 - 4.625,P < 0.001),与参考组相比,高尿量(≥2.0 ml/kg/h)也是30天死亡率的显著危险因素(未调整的OR = 2.069,95%CI:1.701 - 2.516,P < 0.001)。在多变量逻辑回归中也显示了相同的结果,经年龄、性别、生命体征、常见合并症和利尿剂使用情况调整后,低尿量的调整后OR为2.023(95%CI:1.693 - 2.417,P < 0.001),高尿量的调整后OR为1.771(95%CI:1.389 - 2.256,P < 0.001)。此外,尿量减少和尿量增加都是90天死亡率、ICU死亡率、医院死亡率、MV使用和血管升压药使用的危险因素。
尿量减少和增加均与短期死亡率显著相关,尿量与死亡率之间的关系呈U形而非线性。