Schamroth Pravda Nili, Mishaev Raffael, Levi Amos, Witberg Guy, Shapira Yaron, Orvin Katia, Barkan Yeela Talmor, Hamdan Ashraf, Sharoni Ram, Perl Leor, Sagie Alexander, Assa Hana Vaknin, Kornowski Ran, Codner Pablo
Department of Cardiology, Rabin Medical Center, Petah Tikva, Israel associated with Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Sackler Faculty of Medicine, Tel Aviv University, Tel Aviv, Israel.
Front Cardiovasc Med. 2022 Apr 26;9:883242. doi: 10.3389/fcvm.2022.883242. eCollection 2022.
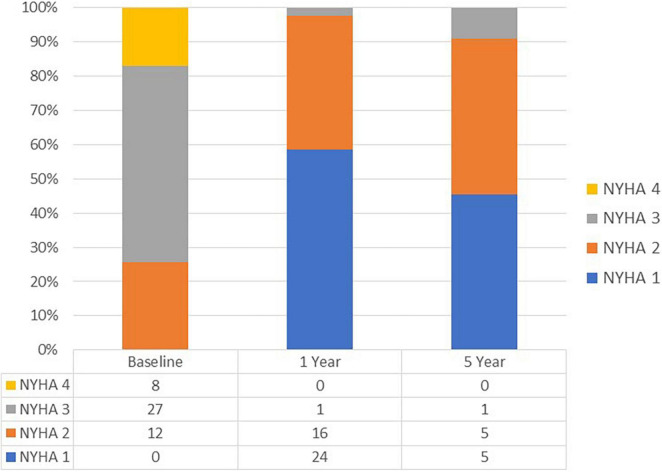
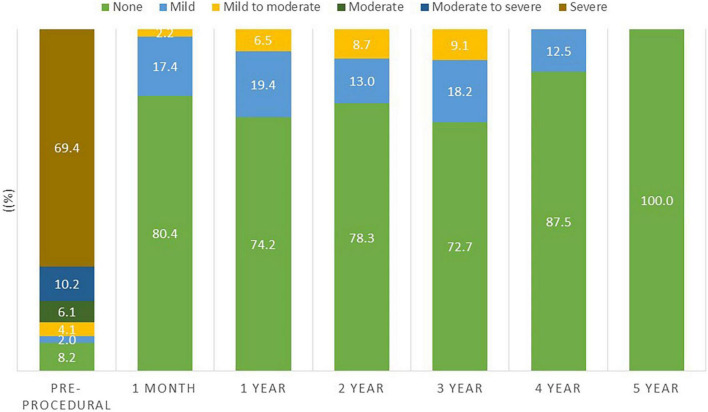
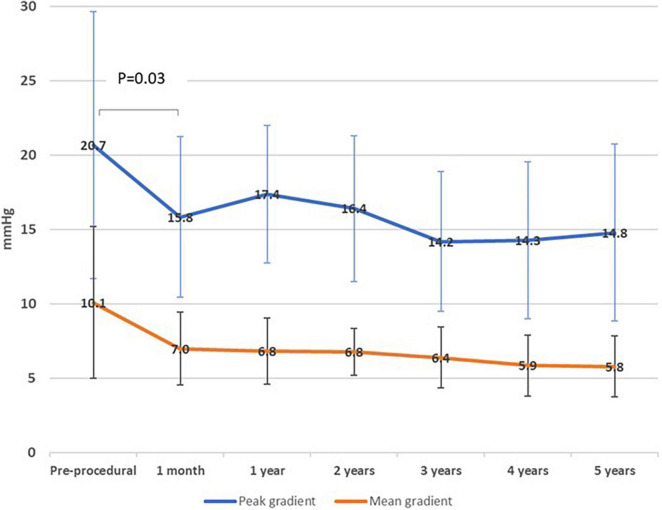
The Valve-in-Valve (ViV) technique is an emerging alternative for the treatment of bioprosthetic structural valve deterioration (SVD) in the mitral position. We report on intermediate-term outcomes of patients with symptomatic SVD in the mitral position who were treated by transcatheter mitral valve-in-valve (TM-ViV) implantation during the years 2010-2019 in our center. Three main outcomes were examined during the follow-up period: NYHA functional class, TM-ViV hemodynamic data per echocardiography, and mortality. Our cohort consisted of 49 patients (mean age 77.4 ± 10.5 years, 65.3% female). The indications for TM-ViV were mainly for regurgitant pathology (77.6%). All 49 patients were treated with a balloon-expandable device. The procedure was performed transapical access in 17 cases (34.7%) and transfemoral vein/trans-atrial septal puncture in 32 cases (65.3%). Mean follow-up was 4.4 ± 2.0 years. 98% and 91% of patients were in NYHA I/II at 1 and 5 years, respectively. Mitral regurgitation was ≥moderate in 86.3% of patients prior to the procedure and this decreased to 0% ( < 0.001) following the procedure and was maintained over 2 years follow-up. The mean trans-mitral valve gradients decreased from pre-procedural values of 10.1 ± 5.1 mmHg to 7.0 ± 2.4 mmHg at 1 month following the procedure ( = 0.03). Mortality at 1 year was 16% (95%, CI 5-26) and 35% (95%, CI 18-49) at 5 years. ViV in the mitral position offers an effective and durable treatment option for patients with SVD at high surgical risk.
瓣中瓣(ViV)技术是治疗二尖瓣位生物瓣结构瓣膜衰败(SVD)的一种新兴替代方法。我们报告了2010年至2019年期间在我们中心接受经导管二尖瓣瓣中瓣(TM-ViV)植入治疗的有症状二尖瓣位SVD患者的中期结果。随访期间检查了三项主要结果:纽约心脏协会(NYHA)心功能分级、每次超声心动图检查的TM-ViV血流动力学数据以及死亡率。我们的队列包括49例患者(平均年龄77.4±10.5岁,65.3%为女性)。TM-ViV的适应症主要为反流性病变(77.6%)。所有49例患者均接受了球囊扩张装置治疗。17例(34.7%)通过经心尖途径进行手术,32例(65.3%)通过经股静脉/经房间隔穿刺进行手术。平均随访时间为4.4±2.0年。分别有98%和91%的患者在1年和5年时处于NYHA I/II级。术前86.3%的患者二尖瓣反流≥中度,术后降至0%(<0.001),并在2年随访期内保持。二尖瓣平均跨瓣压差从术前的10.1±5.1 mmHg降至术后1个月时的7.0±2.4 mmHg(P = 0.03)。1年时的死亡率为16%(95%CI 5-26),5年时为35%(95%CI 18-49)。二尖瓣位ViV为手术风险高的SVD患者提供了一种有效且持久的治疗选择。