Jiang Tao, Huang Bingyu, Huo Shengqi, Mageta Lulu Monica, Guo Junyi, Lv Jiagao, Lin Li
Division of Cardiology, Department of Internal Medicine, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
Front Surg. 2022 Apr 26;9:859205. doi: 10.3389/fsurg.2022.859205. eCollection 2022.
Septal myectomy (SM) has been the gold standard therapy for most patients with hypertrophic obstructive cardiomyopathy (HOCM). Endocardial radiofrequency ablation of septal hypertrophy (ERASH) is a novel treatment for septal reduction. We aimed to assess the efficacy and safety between two treatment strategies.
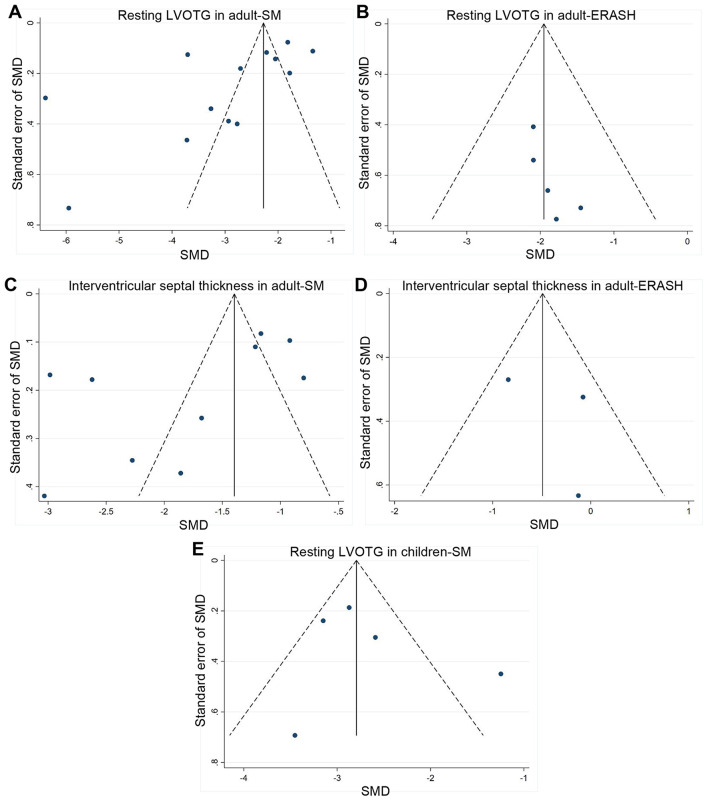
We searched PubMed, Web of Science, Cochrane Library, and Embase databases to identify relevant studies published up to March 2021. Random-effect models were used to calculate standardized mean difference (SMD) and 95% confidence intervals (CIs) for resting left ventricular outflow tract gradient (LVOTG) and septal thickness.
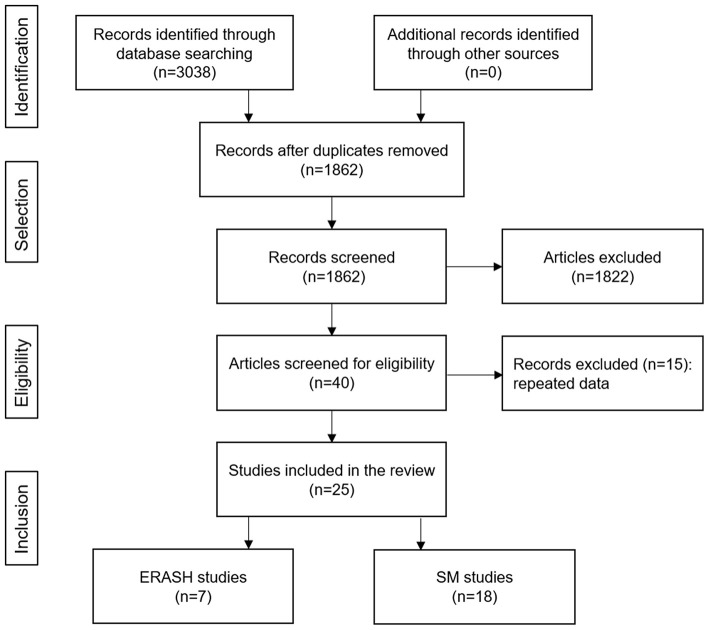
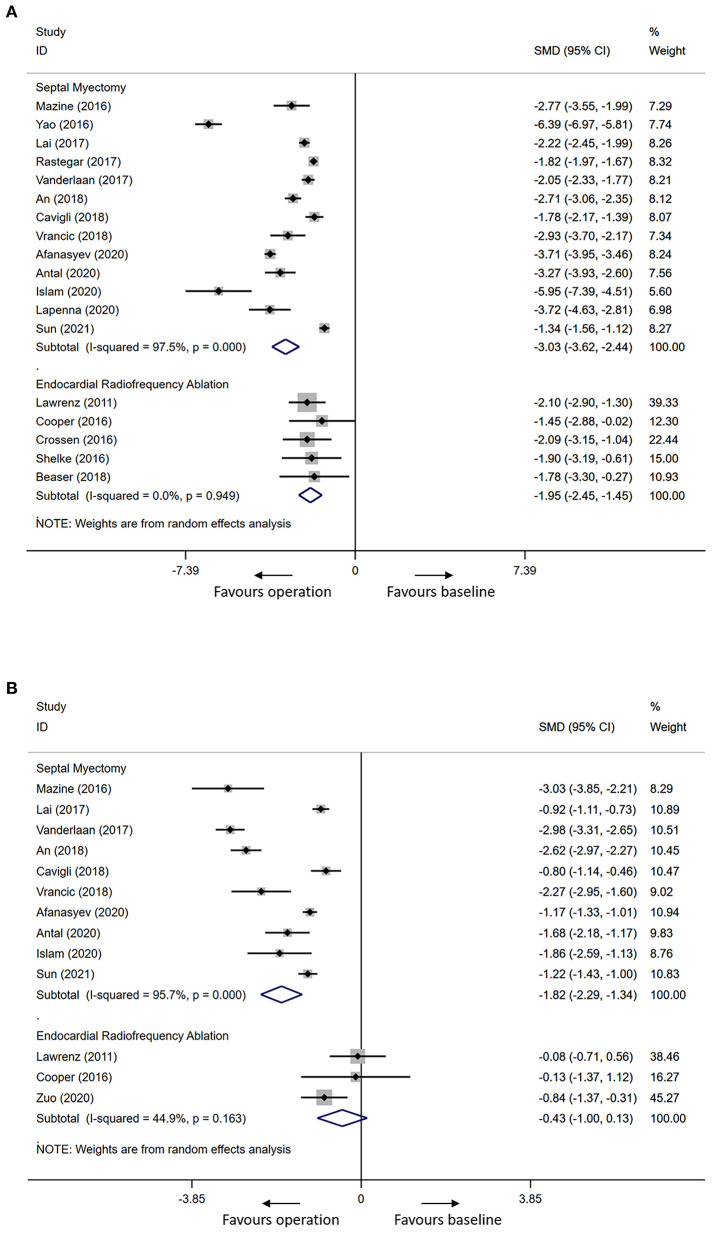
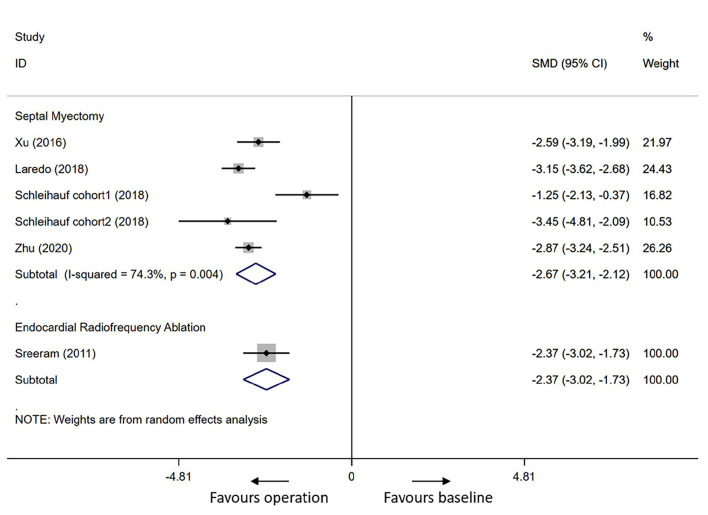
Twenty-five studies are included in this review, eighteen studies for SM and seven studies for ERASH. During follow-up, there were significant reductions of the mean resting LVOTG in adults (SM groups: SMD = -3.03, 95% CI [-3.62 to -2.44]; ERASH groups: SMD = -1.95, 95% CI [-2.45 to -1.45]) and children (SM groups: SMD = -2.67, 95% CI [-3.21 to -2.12]; ERASH groups: SMD= -2.37, 95% CI [-3.02 to -1.73]) after the septal reduction therapies. For adults, SM groups contributed to more obvious reduction than ERASH groups in interventricular septal thickness (SM groups: SMD = -1.82, 95% CI [-2.29 to -1.34]; ERASH groups: SMD = -0.43, 95% CI [-1.00 to 0.13]). The improvement of the New York Heart Association class was similar in the two groups (SM groups: 46.4%; ERASH groups: 46.7%). The periprocedural mortality in SM and ERASH were 1.1 and 1.8%, respectively.
This systematic review suggests that SM is superior to ERASH in the treatment of HOCM. But for the patients who are at risk for open cardiac surgeries or prefer a less invasive approach, ERASH might be an optional approach.
对于大多数肥厚型梗阻性心肌病(HOCM)患者而言,室间隔心肌切除术(SM)一直是金标准治疗方法。经心内膜射频消融肥厚间隔(ERASH)是一种用于间隔减容的新型治疗方法。我们旨在评估两种治疗策略的疗效和安全性。
我们检索了PubMed、科学网、Cochrane图书馆和Embase数据库,以识别截至2021年3月发表的相关研究。采用随机效应模型计算静息左心室流出道梯度(LVOTG)和间隔厚度的标准化平均差(SMD)及95%置信区间(CIs)。
本综述纳入了25项研究,其中18项关于SM,7项关于ERASH。随访期间,成人(SM组:SMD = -3.03,95% CI [-3.62至-2.44];ERASH组:SMD = -1.95,95% CI [-至-1.45])和儿童(SM组:SMD = -2.67,95% CI [-3.21至-2.12];ERASH组:SMD = -2.37,95% CI [-3.02至-1.73])在间隔减容治疗后静息LVOTG均显著降低。对于成人,SM组在室间隔厚度方面的降低比ERASH组更明显(SM组:SMD = -1.82,95% CI [-2.29至-1.34];ERASH组:SMD = -0.43,95% CI [-1.00至0.13])。两组纽约心脏协会心功能分级的改善情况相似(SM组:46.4%;ERASH组:46.7%)。SM和ERASH的围手术期死亡率分别为1.1%和1.8%。
本系统综述表明,在治疗HOCM方面,SM优于ERASH。但对于有心脏直视手术风险或倾向于侵入性较小方法的患者,ERASH可能是一种可选方法。