Su Yi-Chia, Wu Chih-Chien, Su Chien-Chou, Hsieh Meng-Che, Cheng Ching-Lan, Kao Yang Yea-Huei
Department of Pharmacy, Kaohsiung Veterans General Hospital, Kaohsiung 813414, Taiwan.
School of Pharmacy, Institute of Clinical Pharmacy and Pharmaceutical Sciences, College of Medicine, National Cheng Kung University, Tainan 701401, Taiwan.
Cancers (Basel). 2022 Apr 24;14(9):2118. doi: 10.3390/cancers14092118.
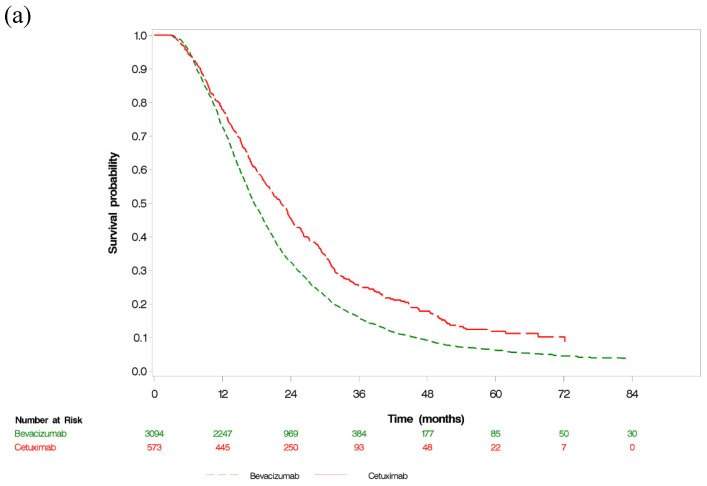
Primary tumor resection may be unfeasible in metastatic colorectal cancer. We determined the effects of bevacizumab and cetuximab therapies on survival or conversion surgery in patients with metastatic colorectal cancer who did not undergo primary tumor resection. This retrospective cohort study enrolled 8466 patients who underwent first-line bevacizumab- or cetuximab-based therapy. We analyzed the data of both therapies in patients who did not undergo primary tumor resection. Overall survival after targeted therapy plus chemotherapy was assessed. The groups were matched using propensity score matching and weighting. Cetuximab resulted in lower mortality than bevacizumab (hazard ratio (HR) = 0.75); however, it did not have the same effect in patients that underwent primary tumor resection (HR = 0.95) after propensity score weighting. Among patients treated with targeted agents, primary tumor resection was associated with lower mortality among those who received both bevacizumab (HR = 0.60) and cetuximab (HR = 0.75). Among patients that did not undergo primary tumor resection, multivariable analysis for conversion surgery showed that the cetuximab group (HR = 1.82) had a significantly higher metastasectomy rate. In these patients, cetuximab-based therapy was associated with significantly better survival compared with bevacizumab-based therapy. Cetuximab also yielded a higher conversion surgery rate. These findings demonstrate the importance of stratification by primary tumor resection in the application of current treatment guidelines and initiation of future clinical trials.
对于转移性结直肠癌,原发性肿瘤切除可能不可行。我们确定了贝伐单抗和西妥昔单抗疗法对未进行原发性肿瘤切除的转移性结直肠癌患者生存或转化手术的影响。这项回顾性队列研究纳入了8466例接受一线贝伐单抗或西妥昔单抗为基础治疗的患者。我们分析了未进行原发性肿瘤切除患者的两种疗法的数据。评估了靶向治疗加化疗后的总生存期。使用倾向评分匹配和加权对各组进行匹配。西妥昔单抗导致的死亡率低于贝伐单抗(风险比(HR)=0.75);然而,在倾向评分加权后,它对接受原发性肿瘤切除的患者没有相同的效果(HR=0.95)。在接受靶向药物治疗的患者中,原发性肿瘤切除与接受贝伐单抗(HR=0.60)和西妥昔单抗(HR=0.75)的患者死亡率较低有关。在未进行原发性肿瘤切除的患者中,转化手术的多变量分析显示西妥昔单抗组(HR=1.82)的转移灶切除率显著更高。在这些患者中,与基于贝伐单抗的治疗相比,基于西妥昔单抗的治疗与显著更好的生存期相关。西妥昔单抗还产生了更高的转化手术率。这些发现证明了在应用当前治疗指南和启动未来临床试验时按原发性肿瘤切除进行分层的重要性。