Department of Hematology, Oncology and Tumor Immunology, CVK, Charité Universitätsmedizin Berlin, Berlin, Germany.
Medical Department III and Comprehensive Cancer Center, Hospital of the University, Ludwig-Maximilian-University (LMU), Munich, Germany.
Ann Surg Oncol. 2020 Jul;27(7):2389-2401. doi: 10.1245/s10434-020-08219-w. Epub 2020 Mar 14.
Tumor assessments after first-line therapy of RAS wild-type mCRC with cetuximab (cet) versus bevacizumab (bev) in combination with FOLFIRI were evaluated for factors influencing resectability, conversion to resectability, and survival after best response.
Conversion to resectability was defined as conversion of initially unresectable to resectable disease at best response as determined by retrospective assessment. Univariate and multivariate logistic models were fitted with resectability at best response as response variable. A Cox model comparing the survival from best response was used to measure the influence of treatment, resectability at best response, and resection. Interaction of resection and treatment arm on survival was tested by likelihood ratio test.
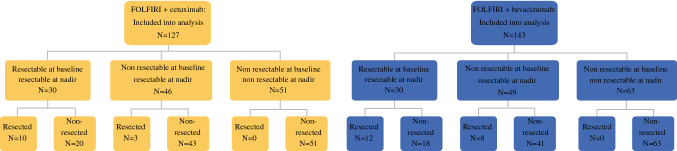
Overall, 270 patients were evaluable (127 cet-arm, 143 bev-arm). Lung metastases (odds ratio [OR] 0.35, 95% confidence response [CI] 0.19-0.63), BRAF mutation (OR 0.33, 95% CI 0.12-0.82), and elevated alkaline phosphatase (OR 0.42, 95% CI 0.18-0.9) before randomization were associated with less chance of successful conversion and were integrated into a nomogram. Early tumor shrinkage (OR 1.86, 95% CI 1.06-3.3; p 0.034) and depth of response (OR 1.02, 95% CI 1.01-1.03; p < 0.001) were associated with successful conversion therapy. Resection of metastases improved post-best-response survival (hazard ratio 0.53, 95% CI 0.29-0.97; p = 0.039), predominantely in cet-treated patients (interaction test, p = 0.02).
Conversion to resectability is significantly associated with baseline characteristics that can be used in a nomogram to predict conversion. Moreover, early efficacy parameters (ETS and DpR) are associated with successful conversion therapy. In FIRE-3, resection of metastases was associated with improved post-best response survival, this effect originated predominantly from the cetuximab-based study arm.
评估 RAS 野生型 mCRC 一线治疗后接受西妥昔单抗(cet)与贝伐珠单抗(bev)联合 FOLFIRI 治疗的肿瘤情况,包括影响可切除性的因素、转化为可切除性的因素以及最佳缓解后的生存情况。
转化为可切除性的定义为根据回顾性评估,在最佳缓解时将最初不可切除的疾病转化为可切除的疾病。使用单变量和多变量逻辑模型,将最佳缓解时的可切除性作为响应变量进行拟合。使用比较最佳缓解时生存情况的 Cox 模型来衡量治疗、最佳缓解时的可切除性和切除的影响。通过似然比检验测试切除和治疗臂对生存的相互作用。
总体而言,270 例患者可评估(127 例 cet 臂,143 例 bev 臂)。随机分组前的肺转移(优势比 [OR] 0.35,95%置信区间 [CI] 0.19-0.63)、BRAF 突变(OR 0.33,95% CI 0.12-0.82)和碱性磷酸酶升高(OR 0.42,95% CI 0.18-0.9)与成功转化的机会较低相关,并被整合到一个列线图中。早期肿瘤缩小(OR 1.86,95% CI 1.06-3.3;p=0.034)和反应深度(OR 1.02,95% CI 1.01-1.03;p<0.001)与成功转化治疗相关。转移灶切除改善了最佳缓解后生存(风险比 0.53,95% CI 0.29-0.97;p=0.039),主要在 cet 治疗组中(交互检验,p=0.02)。
转化为可切除性与基线特征显著相关,这些特征可用于列线图预测转化。此外,早期疗效参数(ETS 和 DpR)与成功的转化治疗相关。在 FIRE-3 中,转移灶切除与最佳缓解后生存改善相关,这种影响主要来源于 cet 治疗组。