Leidi Antonio, Bex Stijn, Righini Marc, Berner Amandine, Grosgurin Olivier, Marti Christophe
Division of General Internal Medicine, Department of Medicine, Geneva University Hospitals, 1205 Geneva, Switzerland.
Division of Angiology and Haemostasis, Department of Medicine, Geneva University Hospitals, 1205 Geneva, Switzerland.
J Clin Med. 2022 Apr 30;11(9):2533. doi: 10.3390/jcm11092533.
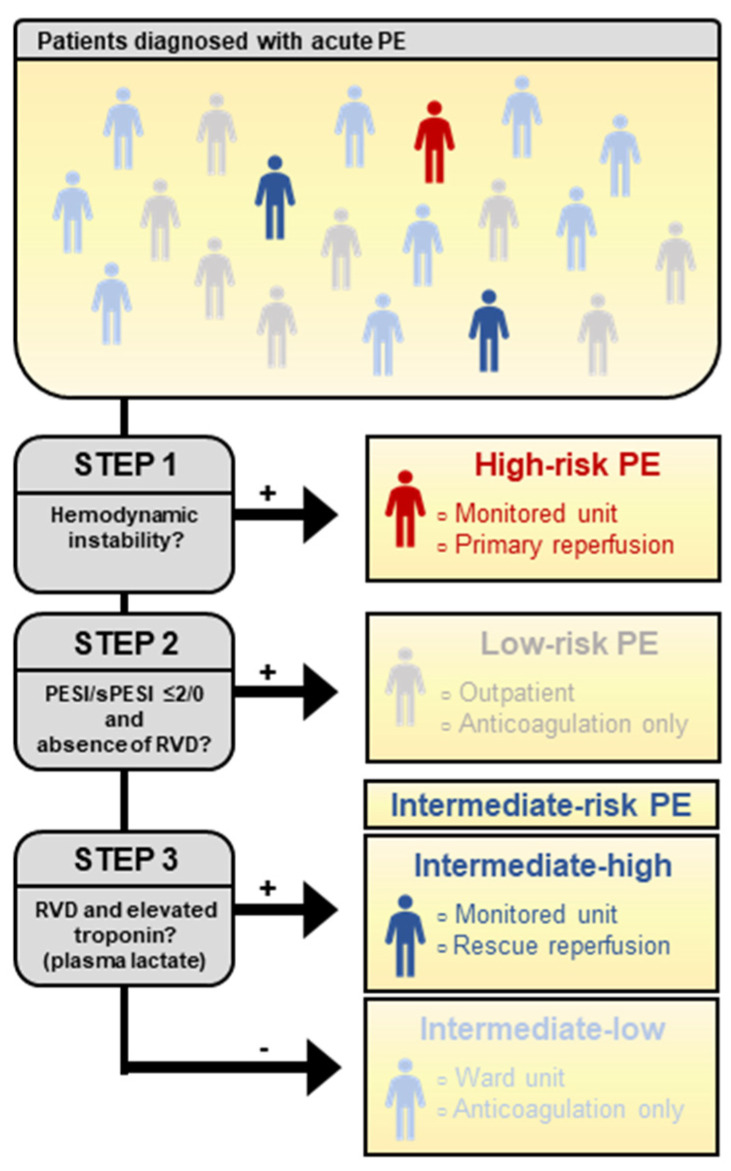
Risk stratification is one of the cornerstones of the management of acute pulmonary embolism (PE) and determines the choice of both diagnostic and therapeutic strategies. The first step is the identification of patent circulatory failure, as it is associated with a high risk of immediate mortality and requires a rapid diagnosis and prompt reperfusion. The second step is the estimation of 30-day mortality based on clinical parameters (e.g., original and simplified version of the pulmonary embolism severity index): low-risk patients without right ventricular dysfunction are safely managed with ambulatory anticoagulation. The remaining group of hemodynamically stable patients, labeled intermediate-risk PE, requires hospital admission, even if most of them will heal without complications. In recent decades, efforts have been made to identify a subgroup of patients at an increased risk of adverse outcomes (intermediate-high-risk PE), who might benefit from a more aggressive approach, including reperfusion therapies and admission to a monitored unit. The cur-rent approach, combining markers of right ventricular dysfunction and myocardial injury, has an insufficient positive predictive value to guide primary thrombolysis. Sensitive markers of circulatory failure, such as plasma lactate, have shown interesting prognostic accuracy and may play a central role in the future. Furthermore, the improved security of reduced-dose thrombolysis may enlarge the indication of this treatment to selected intermediate-high-risk PE.
风险分层是急性肺栓塞(PE)管理的基石之一,决定了诊断和治疗策略的选择。第一步是识别存在血流动力学障碍,因为其与即刻死亡的高风险相关,需要快速诊断和及时再灌注。第二步是根据临床参数(如肺栓塞严重程度指数的原始版本和简化版本)评估30天死亡率:无右心室功能障碍的低风险患者可通过门诊抗凝安全管理。其余血流动力学稳定的患者,标记为中风险PE,需要住院治疗,即使他们中的大多数人将无并发症地康复。近几十年来,人们努力识别出不良结局风险增加的患者亚组(中高风险PE),他们可能从更积极的方法中获益,包括再灌注治疗和入住监护病房。目前结合右心室功能障碍和心肌损伤标志物的方法,其阳性预测价值不足以指导初始溶栓治疗。循环衰竭的敏感标志物,如血浆乳酸,已显示出有趣的预后准确性,可能在未来发挥核心作用。此外,降低剂量溶栓治疗安全性的提高可能会将这种治疗的适应证扩大到选定的中高风险PE。