Department of Orthopedics Surgery, Bone and Joint Research Center, Chang Gung Memorial Hospital, Chang Gung University, No.5, Fu-Shin Street Kweishian, Taoyuan, 333, Taiwan.
J Orthop Surg Res. 2022 May 14;17(1):271. doi: 10.1186/s13018-022-03173-7.
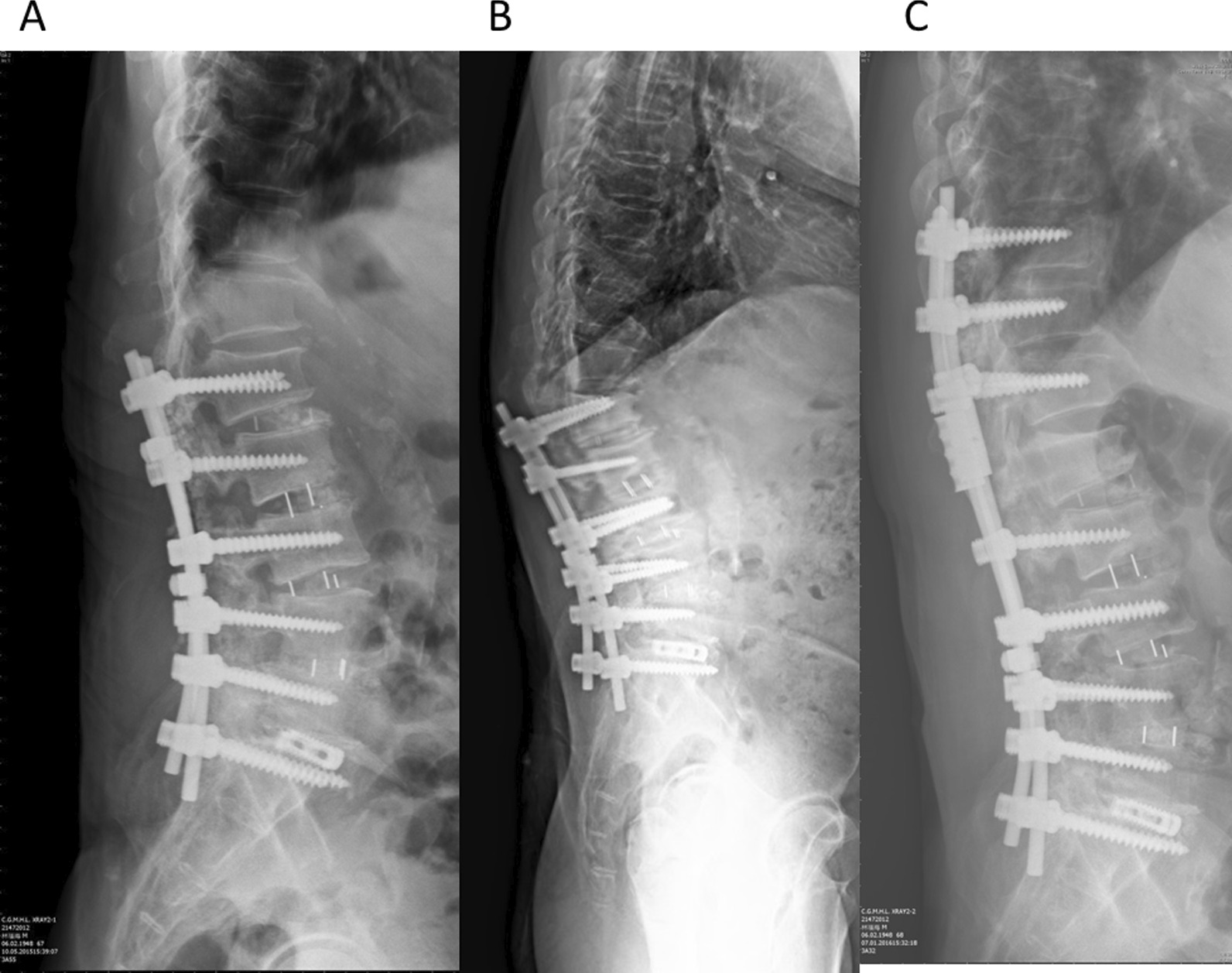
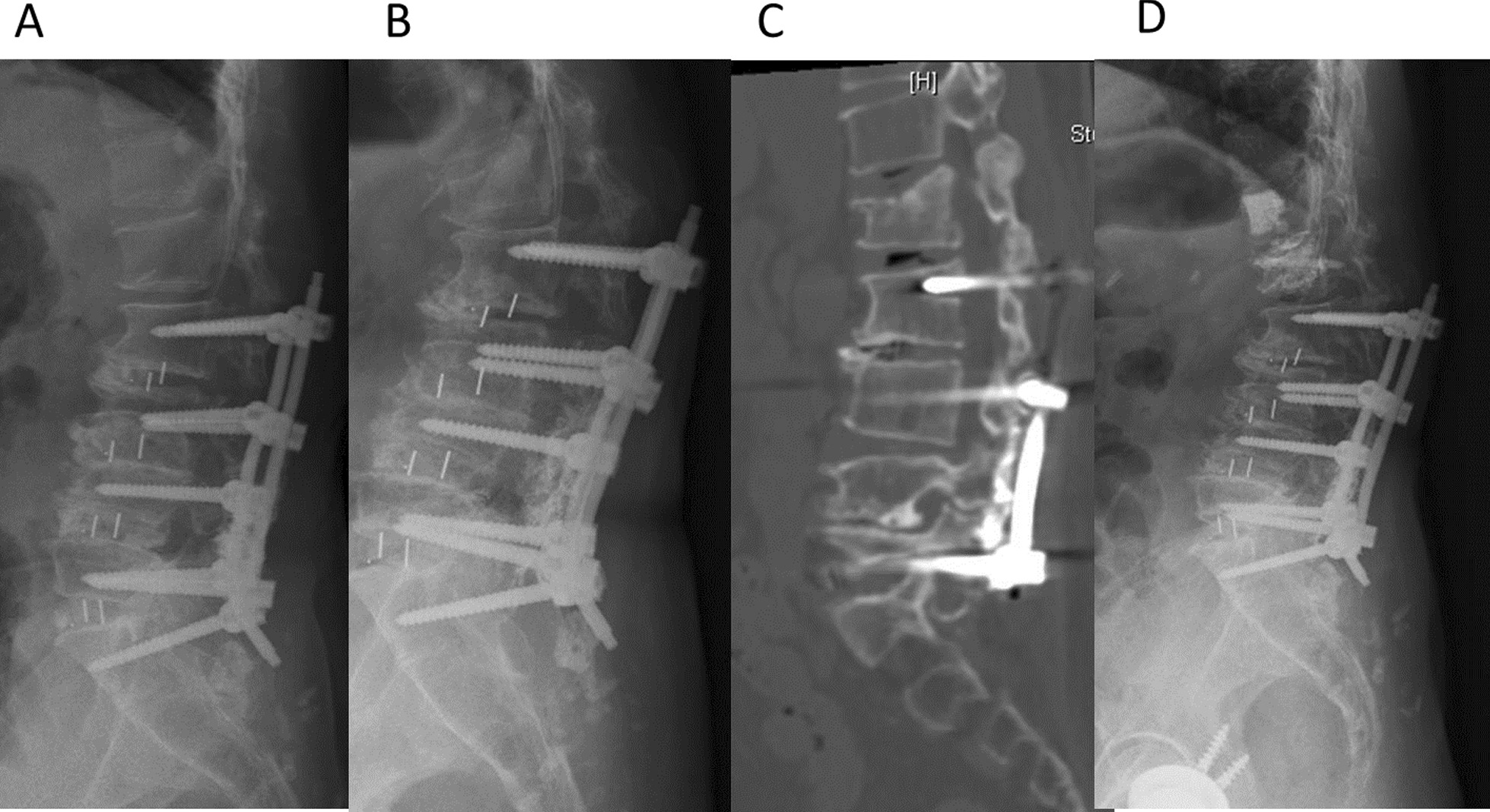
Proximal junctional failure (PJF) is a well-known complication after long-segment (at least 4 vertebral levels) instrumented fusion. The etiologies of PJF include degenerative processes or are fracture induced. The fracture type of PJF includes vertebral fractures developed at the upper instrumented vertebrae (UIV) or UIV + 1. The purpose of this study was to investigate clinical and radiographic features of these two subtypes of PJF and to analyze risk factors in these patients.
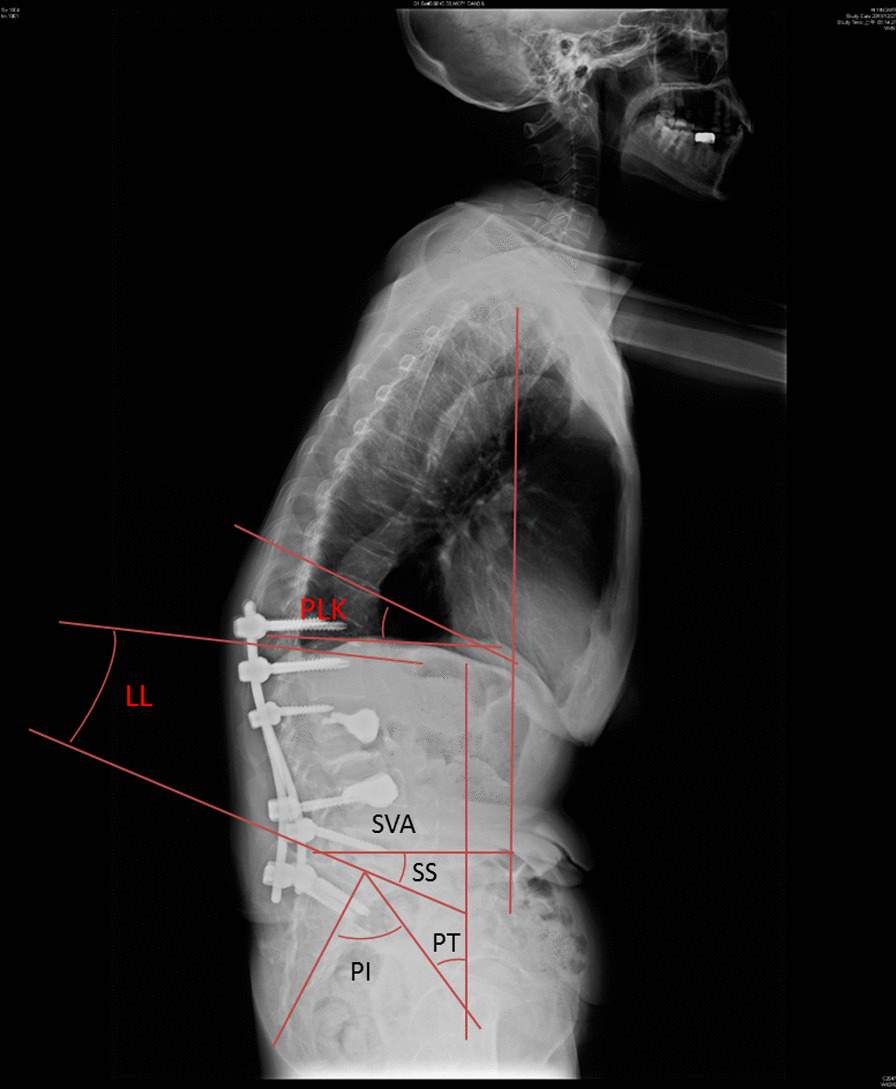
In total, forty-two patients with PJF who underwent revision surgery were included. Twenty patients suffered fractures at the UIV, and the other 22 cases had fractures at UIV + 1. The weighted Charlson Comorbidity Index (CCI) and bone mineral density (BMD) T scores for these patients were recorded. Surgery-related data of index surgery and complications were collected. Radiographic parameters including pelvic tilt (PT), pelvic incidence (PI), sagittal vertical axis (SVA), lumbar lordosis (LL), and PI-LL were recorded in both groups before and after the revision surgery.
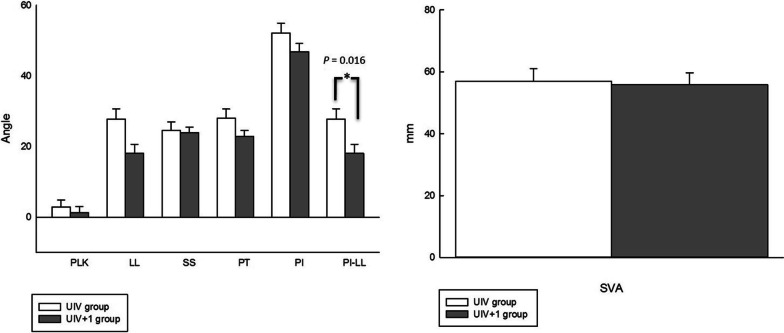
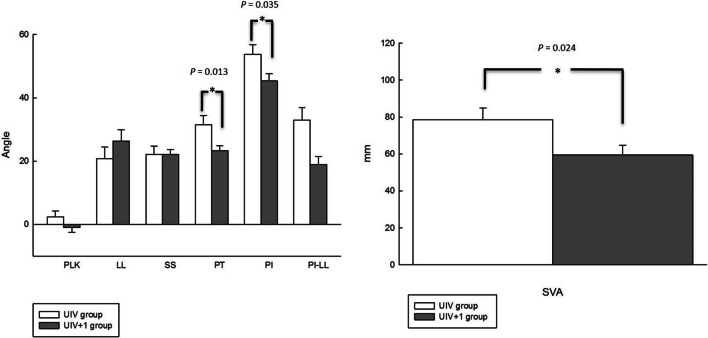
Both groups had severe osteoporosis and comorbidities. The interval between the index surgery and revision surgery was shorter in the UIV group than in the UIV + 1 group (8.2 months vs. 35.9 months; p < 0.001). The analysis for radiographic parameters in UIV and UIV + 1 group demonstrated no significant change before and after the revision surgery. However, the preoperative radiographic analysis showed a larger PT (31.5° vs. 23.2°, p = 0.013), PI (53.7° vs. 45.3°, p = 0.035), and SVA (78.6° vs. 59.4°, p = 0.024) in the UIV group compared to the UIV + 1 group. The postoperative radiographic analysis showed a larger PI-LL (27.8° vs. 18.1°, p = 0.016) in the UIV group compared to the UIV + 1 group.
PJF in the UIV group tends to occur earlier than in the UIV + 1 group. Moreover, more severe global sagittal imbalances were found in the UIV group than in UIV + 1 group.
近端交界性失败(PJF)是长节段(至少 4 个椎体水平)器械融合后一种常见的并发症。PJF 的病因包括退行性过程或骨折引起。PJF 的骨折类型包括在上固定椎体(UIV)或 UIV+1 处发生的椎体骨折。本研究的目的是探讨这两种亚型 PJF 的临床和影像学特征,并分析这些患者的危险因素。
共纳入 42 例接受翻修手术的 PJF 患者。20 例患者 UIV 处发生骨折,另 22 例患者 UIV+1 处发生骨折。记录这些患者的加权 Charlson 合并症指数(CCI)和骨密度(BMD)T 评分。收集索引手术和并发症的手术相关数据。在两组患者翻修术前和术后记录骨盆倾斜角(PT)、骨盆入射角(PI)、矢状垂直轴(SVA)、腰椎前凸角(LL)和 PI-LL 等影像学参数。
两组患者均有严重的骨质疏松症和合并症。UIV 组索引手术与翻修手术的间隔时间短于 UIV+1 组(8.2 个月 vs. 35.9 个月;p<0.001)。UIV 和 UIV+1 组影像学参数的分析显示,翻修前后无明显变化。然而,术前影像学分析显示 UIV 组的 PT(31.5° vs. 23.2°,p=0.013)、PI(53.7° vs. 45.3°,p=0.035)和 SVA(78.6° vs. 59.4°,p=0.024)大于 UIV+1 组。术后影像学分析显示 UIV 组的 PI-LL(27.8° vs. 18.1°,p=0.016)大于 UIV+1 组。
UIV 组的 PJF 比 UIV+1 组更容易发生。此外,UIV 组的整体矢状失平衡比 UIV+1 组更严重。