NHMRC Clinical Trials Centre, the University of Sydney, Camperdown, NSW, 2050, Australia.
Australian Research Centre for Population Oral Health, The University of Adelaide, Adelaide, Australia.
BMC Public Health. 2022 May 14;22(1):971. doi: 10.1186/s12889-022-13338-y.
Aboriginal and Torres Strait Islander peoples (hereafter respectfully referred to as Indigenous Australians) represent about 3% of the total Australian population. Major health disparities exist between Indigenous and Non-Indigenous Australians. To address this, it is vital to understand key health priorities and knowledge gaps in the current landscape of clinical trial activity focusing on Indigenous health in Australia.
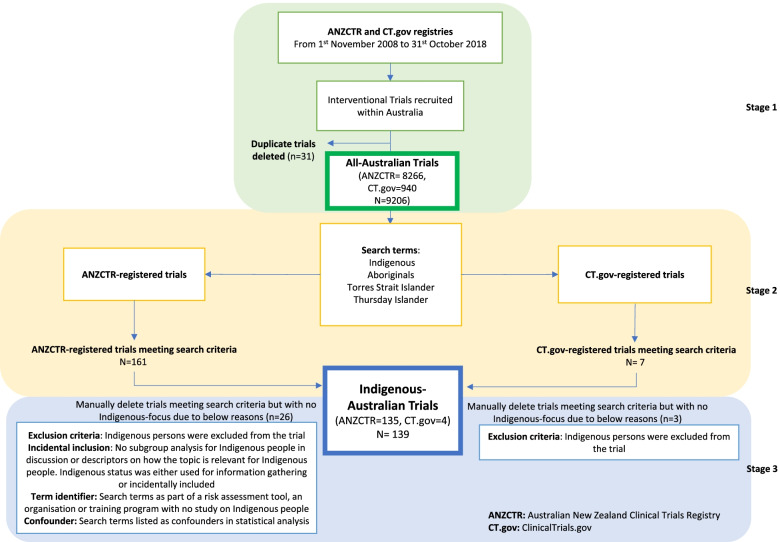
Australian-based clinical trials registered on the Australian New Zealand Clinical Trials Registry or ClinicalTrials.gov from 2008 to 2018 were analysed. Australian clinical trials with and without a focus on Indigenous health were compared in terms of total numbers, participant size, conditions studied, design, intervention type and funding source.
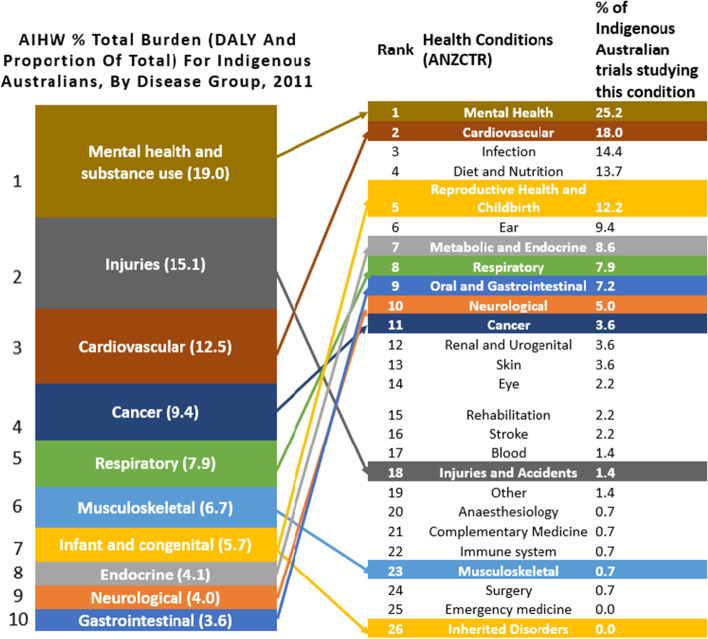
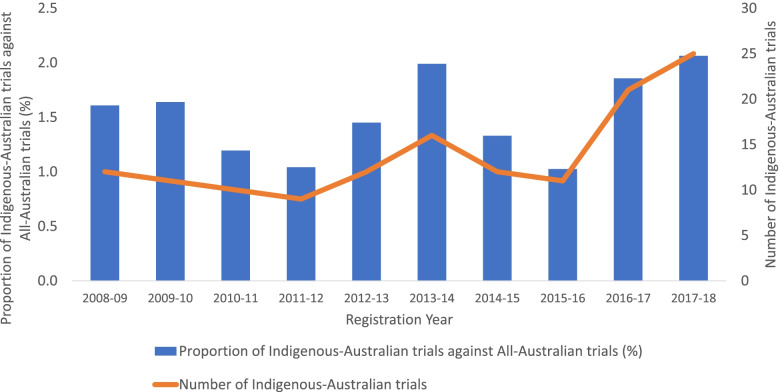
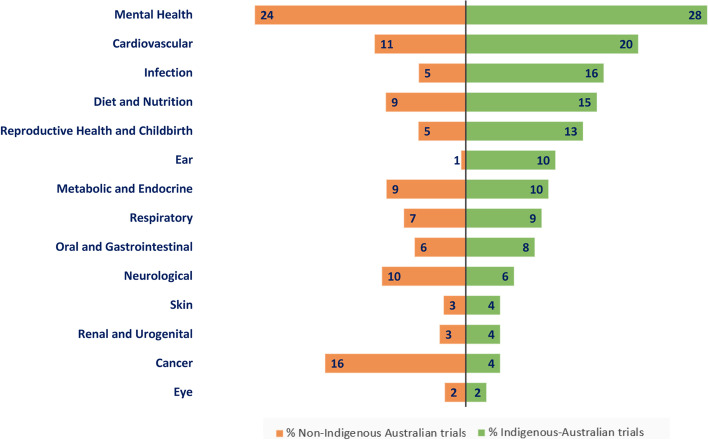
Of the 9206 clinical trials included, 139 (1.5%) focused on Indigenous health, with no proportional increase in Indigenous trials over the decade (p = 0.30). Top conditions studied in Indigenous-focused trials were mental health (n = 35, 28%), cardiovascular disease (n = 20, 20%) and infection (n = 16, 16%). Compared to General Australian trials, Indigenous-focused trials more frequently studied ear conditions (OR 20.26, 95% CI 10.32-37.02, p < 0.001), infection (OR 3.11, 95% CI 1.88-4.85, p < 0.001) and reproductive health (OR 2.59, 95% CI 1.50-4.15, p < 0.001), and less of musculoskeletal conditions (OR 0.09, 95% CI 0.00-0.37, p < 0.001), anaesthesiology (OR 0.16, 95% CI 0.01-0.69, p = 0.021) and surgery (OR 0.17, 95% CI 0.01-0.73, p = 0.027). For intervention types, Indigenous trials focused more on prevention (n = 48, 36%) and screening (n = 18, 13%). They were far less involved in treatment (n = 72, 52%) as an intervention than General Australian trials (n = 6785, 75%), and were less likely to be blinded (n = 48, 35% vs n = 4273, 47%) or have industry funding (n = 9, 7% vs 1587, 17%).
Trials with an Indigenous focus differed from General Australian trials in the conditions studied, design and funding source. The presented findings may inform research prioritisation and alleviate the substantial burden of disease for Indigenous population.
澳大利亚原住民和托雷斯海峡岛民(以下简称澳大利亚原住民)约占澳大利亚总人口的 3%。原住民和非原住民之间存在重大健康差距。为了解决这个问题,了解澳大利亚目前关注原住民健康的临床试验活动的主要优先事项和知识空白至关重要。
对 2008 年至 2018 年在澳大利亚新西兰临床试验注册处或 ClinicalTrials.gov 注册的澳大利亚临床试验进行分析。对有和没有关注原住民健康的澳大利亚临床试验在总数、参与者规模、研究的疾病、设计、干预类型和资金来源方面进行了比较。
在纳入的 9206 项临床试验中,有 139 项(1.5%)关注原住民健康,但在十年内原住民试验没有呈比例增加(p=0.30)。在关注原住民健康的试验中,研究最多的疾病是心理健康(n=35,28%)、心血管疾病(n=20,20%)和感染(n=16,16%)。与澳大利亚一般试验相比,关注原住民健康的试验更频繁地研究耳部疾病(OR 20.26,95%CI 10.32-37.02,p<0.001)、感染(OR 3.11,95%CI 1.88-4.85,p<0.001)和生殖健康(OR 2.59,95%CI 1.50-4.15,p<0.001),较少研究肌肉骨骼疾病(OR 0.09,95%CI 0.00-0.37,p<0.001)、麻醉学(OR 0.16,95%CI 0.01-0.69,p=0.021)和手术(OR 0.17,95%CI 0.01-0.73,p=0.027)。就干预类型而言,原住民试验更侧重于预防(n=48,36%)和筛查(n=18,13%)。它们作为干预措施参与治疗的比例远低于澳大利亚一般试验(n=6785,75%),而且不太可能进行盲法(n=48,35%比 n=4273,47%)或获得行业资助(n=9,7%比 n=1587,17%)。
关注原住民的试验在研究的疾病、设计和资金来源方面与澳大利亚一般试验不同。提出的研究结果可能为研究重点提供信息,并减轻原住民人口的疾病负担。