Department of Anesthesiology, Xuzhou Central Hospital, The Affiliated XuZhou Hospital of Nanjing Medical University, Suzhou, China.
Department of Cardiology, The Affiliated Suzhou Hospital of Nanjing Medical University, Suzhou Municipal Hospital, Gusu School, Nanjing Medical University, Suzhou, China.
Clin Transl Sci. 2022 Aug;15(8):1926-1936. doi: 10.1111/cts.13304. Epub 2022 May 28.
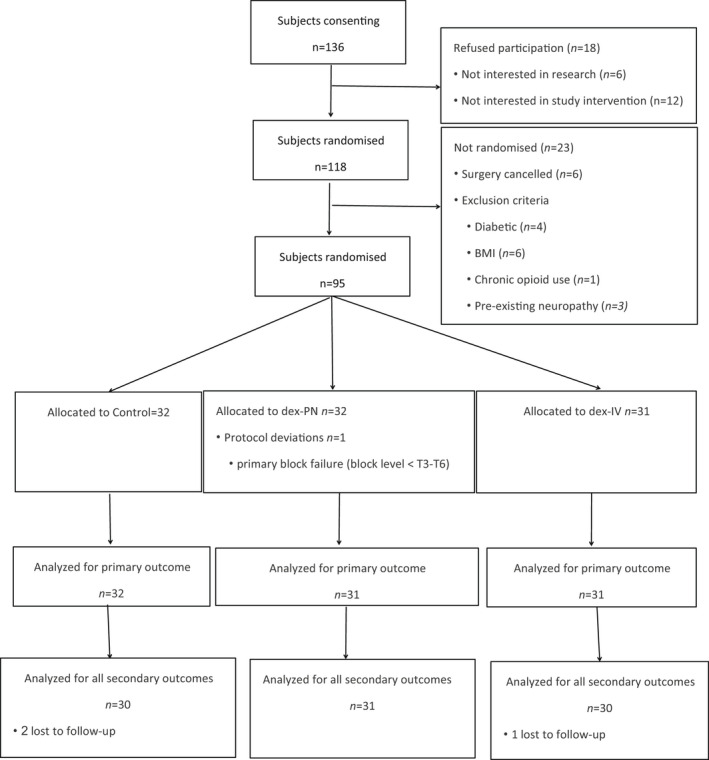
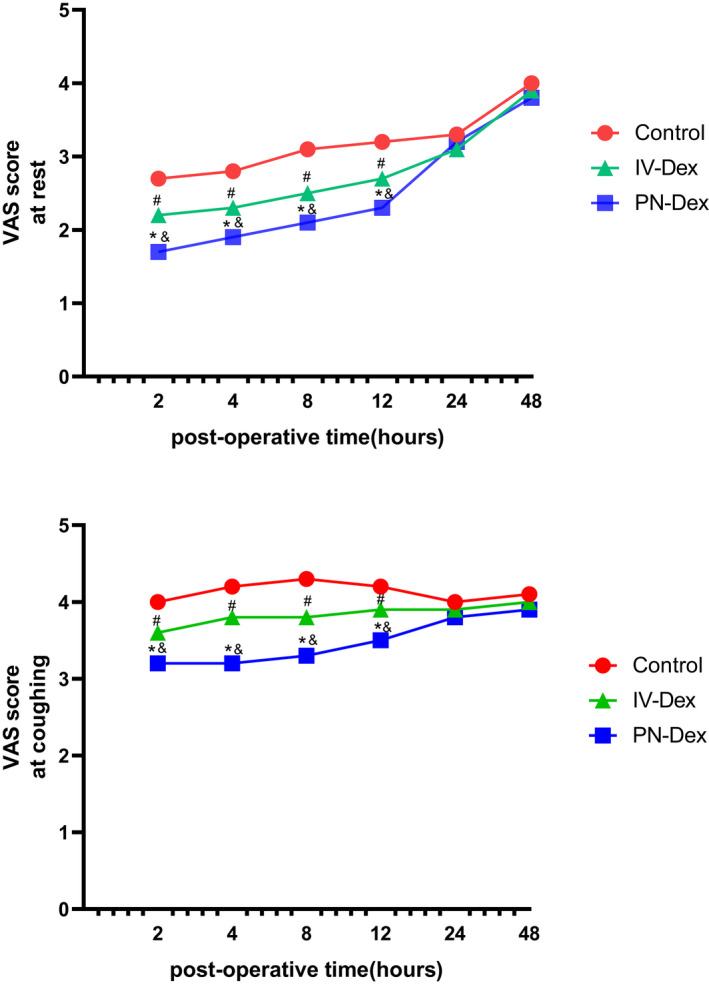
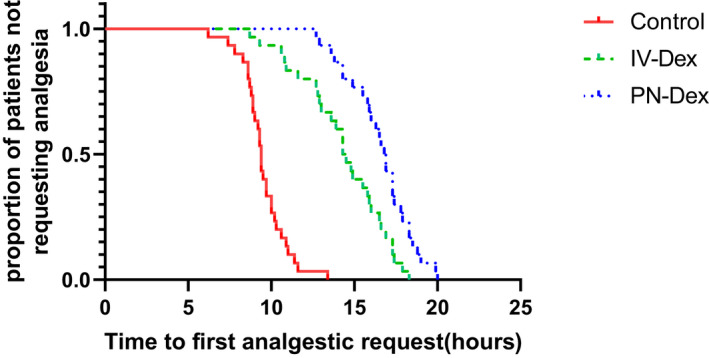
Efforts to prolong thoracic paravertebral block (TPVB) analgesia include local anesthetic adjuvants, such as dexamethasone (Dex). Previous studies showed that both perineural (PN) and intravenous (i.v.) routes could prolong analgesia. As PN Dex is an off-label use, anesthesiologists should be fully informed of the clinical differences, if any, on block duration. This study was designed to evaluate the two administration routes of Dex for duration of analgesia in TPVB. Ninety-five patients scheduled for Ivor-Lewis esophagectomy were randomized to receive TPVB (0.5% ropivacaine 15 ml), PN or i.v. Dex 8 mg. The primary end point was the duration of analgesia. The secondary end points included pain scores, analgesic consumption, adverse effects rate, and incidence of chronic pain at 3 months postoperatively. The PN-Dex group showed better analgesic effects than the i.v.-Dex group (p < 0.05). Similarly, the visual analogue scale scores in patients at 2, 4, 8, and 12 h postoperatively were lower in the PN-Dex group than the i.v.-Dex group (p < 0.05). The analgesic consumption in both the PN-Dex and i.v.-Dex groups was significantly lower than that in the control group (p < 0.05). Regarding the incidence of chronic pain, regardless of route, Dex decreased the incidence of chronic postsurgical pain and neuropathic pain at 3 months after surgery (p < 0.05), but there were no clinical differences between the i.v.-Dex and PN-Dex groups. Perineural dexamethasone improved the magnitude and duration of analgesia compared to that of the i.v.-Dex group in TPVB in Ivor-Lewis esophagectomy. However, there were no clinically significant differences between the two groups in the incidence of chronic pain.
为延长胸段椎旁阻滞(TPVB)镇痛时间,可加入局部麻醉药佐剂,如地塞米松(Dex)。既往研究表明,经外周神经(PN)和静脉(iv.)途径均可延长镇痛时间。由于 PN 给予 Dex 为超说明书用药,麻醉医生应充分了解两种途径在阻滞持续时间上的临床差异。本研究旨在评估 PN 和 iv. 给予 Dex 对 TPVB 中镇痛持续时间的影响。95 例行 Ivor-Lewis 食管癌切除术的患者随机分为三组,分别接受 TPVB(0.5%罗哌卡因 15ml)、PN 或 iv. 给予 Dex 8mg。主要终点为镇痛持续时间。次要终点包括疼痛评分、镇痛药用量、不良反应发生率以及术后 3 个月慢性疼痛发生率。PN-Dex 组镇痛效果优于 iv.-Dex 组(p<0.05)。同样,PN-Dex 组患者术后 2、4、8 和 12h 的视觉模拟评分(VAS)均低于 iv.-Dex 组(p<0.05)。PN-Dex 和 iv.-Dex 组的镇痛药用量均显著低于对照组(p<0.05)。无论给药途径如何,Dex 均降低了术后 3 个月慢性术后痛和神经病理性疼痛的发生率(p<0.05),但 iv.-Dex 组与 PN-Dex 组之间无临床差异。与 iv.-Dex 组相比,PN 给予 Dex 可提高食管癌 Ivor-Lewis 手术中 TPVB 的镇痛效果和持续时间。然而,两组慢性疼痛的发生率无显著差异。