Early Detection, Prevention and Infections Branch, International Agency for Research on Cancer (IARC/WHO), Lyon, France.
Early Detection, Prevention and Infections Branch, International Agency for Research on Cancer (IARC/WHO), Lyon, France.
Lancet Gastroenterol Hepatol. 2022 Aug;7(8):724-735. doi: 10.1016/S2468-1253(22)00050-4. Epub 2022 May 14.
Empirical, updated country-level estimates on the proportion of cirrhosis attributable to viral hepatitis are required. We estimated the prevalence of hepatitis B virus (HBV) and hepatitis C virus (HCV) infection in patients with cirrhosis at country, regional, and global levels as an approximation for the fractions of cirrhosis attributable to viral hepatitis.
In this systematic review, we searched MEDLINE, Embase, Web of Science, and Scielo between Jan 1, 1993, and Aug 1, 2021. Studies were eligible if they reported on the prevalence of both HBV and HCV infection in representative studies of at least 20 patients with cirrhosis. Studies were excluded if they used first-generation HCV assays or were from a selected population of patients with cirrhosis (eg, patients selected based on specific causes, veterans, injecting drug users). Two authors (CJA and CdM) selected and extracted aggregated data from the selected publications. Data were extracted for study recruitment period, age, sex, and cause of cirrhosis, among others. Data about heavy alcohol consumption and non-alcoholic fatty liver disease (NAFLD) were also extracted when available. Aggregated data from studies from key publications were requested from the authors of the original study if selection of patients was unclear or information on causes was missing. We estimated the country-specific prevalence of causes of cirrhosis by pooling study-level data from the same country using a random-effects model. Subsequently, we estimated the regional (WHO region and UN subregion) and global prevalence by weighting the country-specific prevalence by the number of new liver cancer cases that occurred in 2020, as estimated in GLOBOCAN. The study was registered with PROSPERO, CRD42020149323.
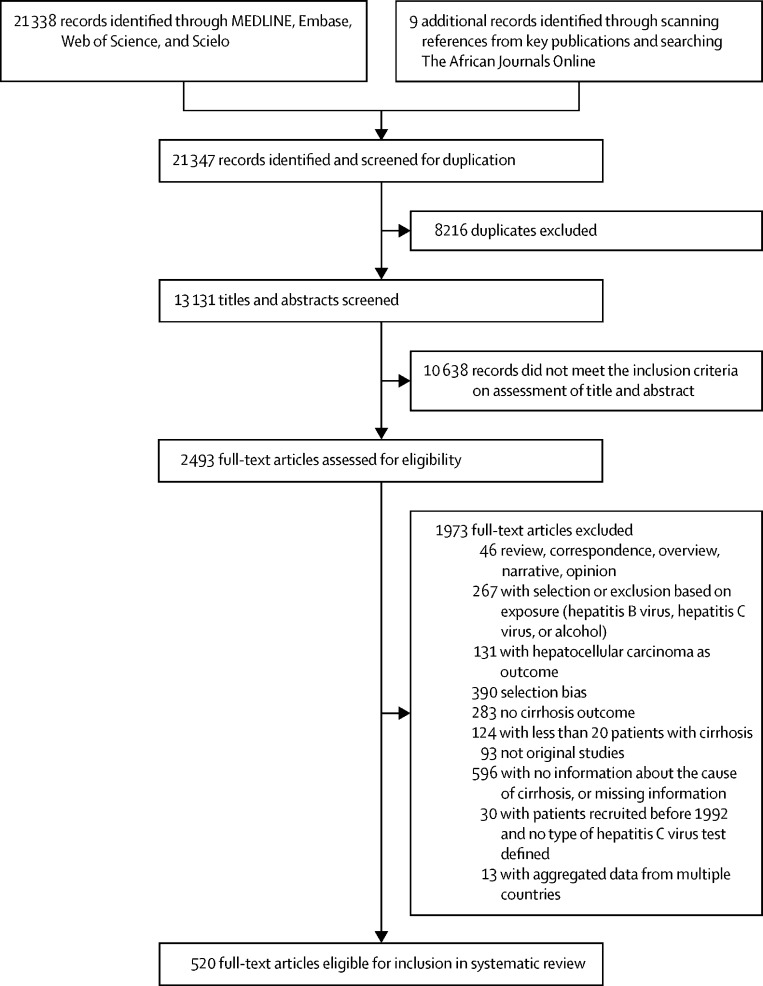
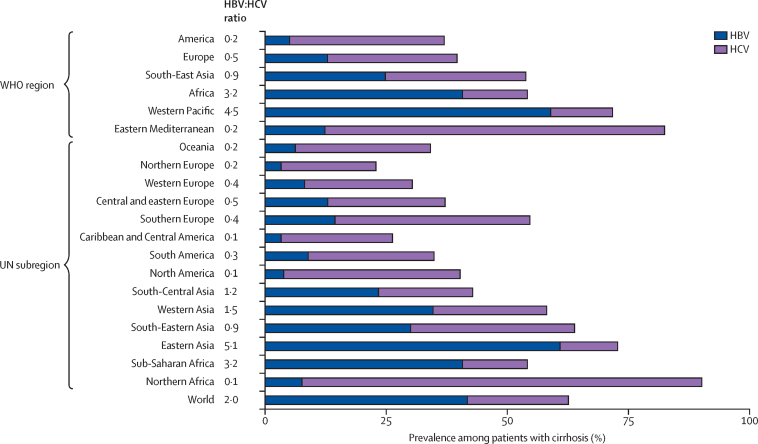
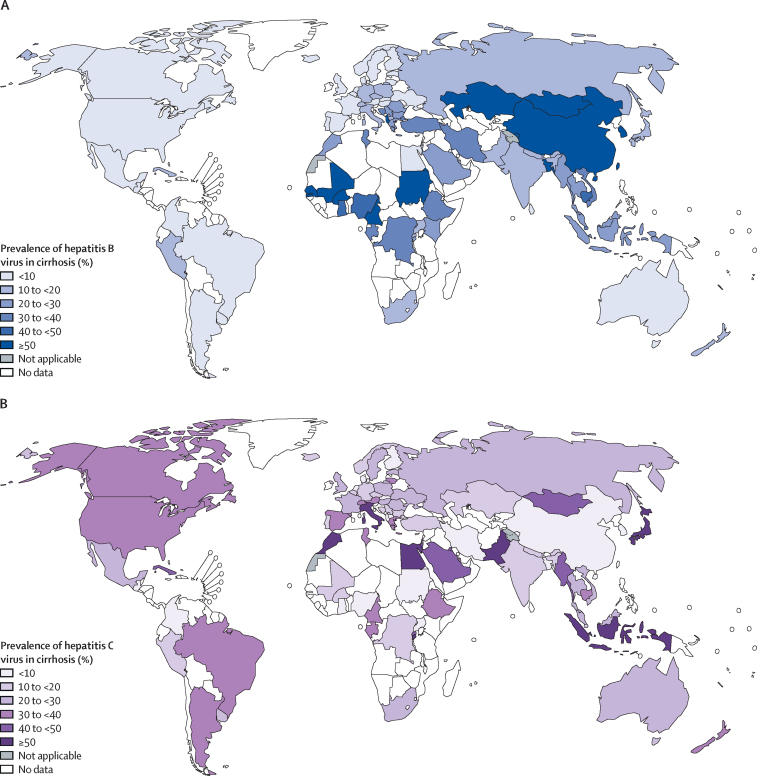
Our database searches identified 21 338 records, and a further nine records were identified by scanning references of key publications. After excluding duplicates and assessing full-text articles for eligibility, 520 publications from 86 countries or territories (and reporting on 1 376 503 patients with cirrhosis) were included in the systematic review. The prevalence of HBV infection was lower among patients with cirrhosis in Europe, the Americas, and Oceania (UN subregional prevalence ranges 3-14%) than in Africa and Asia (8-61%). HCV infection prevalence was heterogenous, even within regions (12-83%). The combined prevalence of HBV and HCV infection exceeded 50% in most Asian and African regions. Globally, among patients with cirrhosis, 42% had HBV infection and 21% had HCV infection. The contribution of heavy alcohol use was highest in Europe (country range 16-78%), the Americas (17-52%), and Oceania (15-37%) and lowest in Asia (0-41%). Data on NAFLD were limited.
HBV and HCV could account for almost two thirds of the global burden of cirrhosis. With the availability of effective interventions for the prevention or treatment of HBV and HCV, the data presented in this study will help to effectively allocate resources towards viral hepatitis elimination and to design interventions at the country level.
International Agency for Research on Cancer, World Health Organization.
需要提供关于病毒性肝炎导致肝硬化的国家层面的经验、最新估计数。我们估算了乙型肝炎病毒(HBV)和丙型肝炎病毒(HCV)在肝硬化患者中的流行程度,这些数据近似于病毒性肝炎导致肝硬化的比例。
在本次系统评价中,我们检索了 1993 年 1 月 1 日至 2021 年 8 月 1 日期间 MEDLINE、Embase、Web of Science 和 Scielo 中的数据。如果研究报告了至少 20 例肝硬化患者的 HBV 和 HCV 感染流行率,并具有代表性,则符合入选标准。如果研究使用第一代 HCV 检测方法或来自特定人群(例如,基于特定病因、退伍军人、静脉吸毒者等选择的患者)的肝硬化患者的选择人群,则予以排除。两位作者(CJA 和 CdM)从入选文献中选择和提取汇总数据。数据提取内容包括研究招募期、年龄、性别和肝硬化病因等。如果有关于大量饮酒和非酒精性脂肪性肝病(NAFLD)的数据,也将提取这些数据。如果患者选择不明确或病因信息缺失,将从原始研究的作者处请求来自关键出版物的汇总数据。我们使用随机效应模型汇总来自同一国家的研究水平数据,估算各国的肝硬化病因特异性流行率。随后,我们根据 2020 年全球癌症数据库(GLOBOCAN)估计的新肝癌病例数,通过为每个国家的流行率赋予权重,估算了区域(世卫组织区域和联合国次区域)和全球流行率。本研究已在 PROSPERO 上注册,注册号为 CRD42020149323。
我们的数据库检索共确定了 21338 条记录,通过扫描关键文献的参考文献又确定了另外 9 条记录。在排除重复项并对全文文章进行资格评估后,从 86 个国家或地区的 520 篇文献(共报告了 1376503 例肝硬化患者)中纳入了本次系统评价。与非洲和亚洲(8%-61%)相比,欧洲、美洲和大洋洲(联合国次区域流行率范围为 3%-14%)肝硬化患者中 HBV 感染率较低。HCV 感染率存在差异,即使在同一区域内也是如此(12%-83%)。在大多数亚洲和非洲地区,HBV 和 HCV 合并感染的流行率超过 50%。全球范围内,42%的肝硬化患者有 HBV 感染,21%的患者有 HCV 感染。在欧洲(国家范围为 16%-78%)、美洲(17%-52%)和大洋洲(15%-37%),大量饮酒的影响最大,而在亚洲(0%-41%),其影响最小。关于 NAFLD 的数据有限。
HBV 和 HCV 可能占全球肝硬化负担的近三分之二。由于有针对 HBV 和 HCV 的有效预防或治疗干预措施,本研究中提供的数据将有助于有效地为病毒性肝炎消除分配资源,并在国家层面设计干预措施。
国际癌症研究机构,世界卫生组织。