Tan Lee A, Yoganandan Narayan, Choi Hoon, Purushothaman Yuvaraj, Jebaseelan Davidson, Bosco Aju
Department of Neurological Surgery, University of California San Francisco, San Francisco, CA, USA.
Department of Neurosurgery, Medical College of Wisconsin, Milwaukee, WI, USA.
Neurospine. 2022 Jun;19(2):385-392. doi: 10.14245/ns.2143230.615. Epub 2022 May 13.
Pseudarthrosis and adjacent segment degeneration (ASD) are 2 common complications after multilevel anterior cervical discectomy and fusion (ACDF). We aim to identify the potential biomechanical factors contributing to pseudarthrosis and ASD following 3-level ACDF using a cervical spine finite element model (FEM).
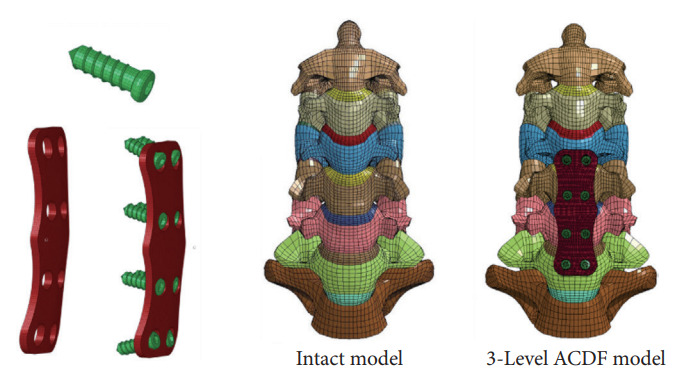
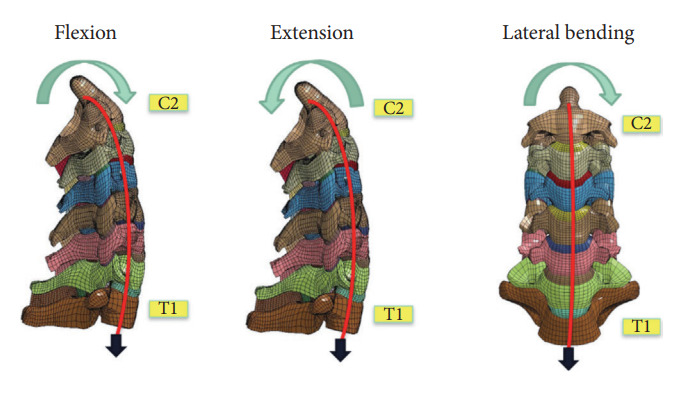
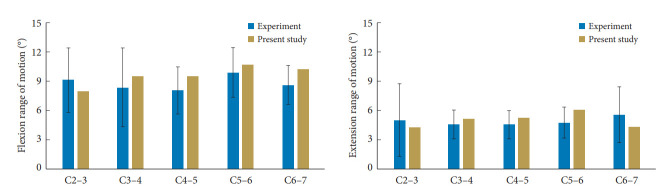
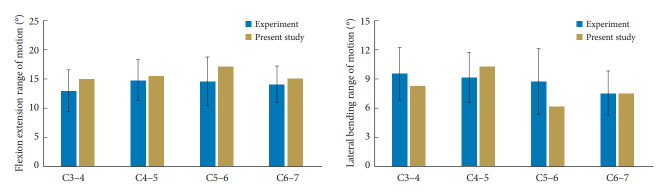
A validated cervical spine FEM from C2 to C7 was used to study the biomechanical factors in cervical spine intervention. The FEM model was used to simulate a 3-level ACDF with intervertebral spacers and anterior cervical plating with screw fixation from C4 to C7. The model was then constrained at the inferior nodes of the T1 vertebra, and physiological loads were applied at the top vertebra. The pure moment load of 2 Nm was applied in flexion, extension, and lateral bending. A follower axial force of 75 N was applied to reproduce the weight of the cranium and muscle force, was applied using standard procedures. The motion-controlled hybrid protocol was utilized to comprehend the adjustments in the spinal biomechanics.
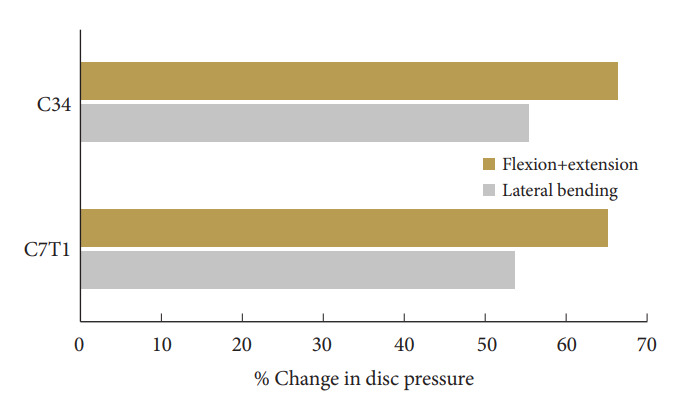
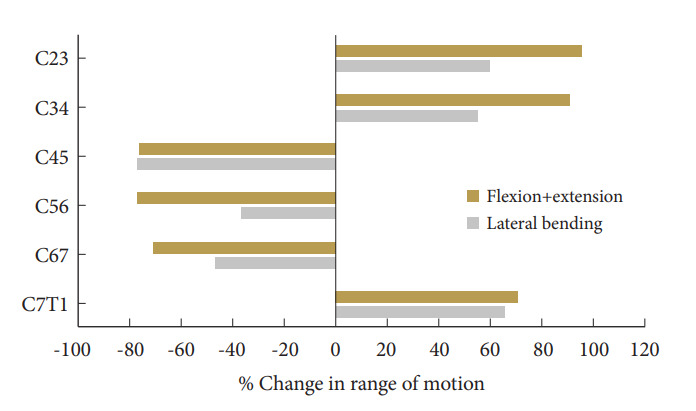
Our cervical spine FEM demonstrated that the cranial adjacent level (C3-4) had significantly more increase in range of motion (ROM) (+90.38%) compared to the caudal adjacent level at C7-T1 (+70.18%) after C4-7 ACDF, indicating that the cranial adjacent level has more compensatory increase in ROM than the caudal adjacent level, potentially predisposing it to earlier ASD. Within the C4-7 ACDF construct, the C6-7 level had the least robust fixation during fixation compared to C4-5 and C5-6, as reflected by the smallest reduction in ROM compared to intact spine (-71.30% vs. -76.36% and -77.05%, respectively), which potentially predisposes the C6-7 level to higher risk of pseudarthrosis.
Biomechanical analysis of C4-7 ACDF construct using a validated cervical spine FEM indicated that the C3-4 has more compensatory increase in ROM compared to C7-T1, and C6-7 has the least robust fixation under physiological loads. These findings can help spine surgeons to predicate the areas with higher risks of pseudarthrosis and ASD, and thus developing corresponding strategies to mitigate these risks and provide appropriate preoperative counseling to patients.
假关节形成和相邻节段退变(ASD)是多节段颈椎前路椎间盘切除融合术(ACDF)后两种常见的并发症。我们旨在使用颈椎有限元模型(FEM)确定导致三节段ACDF术后假关节形成和ASD的潜在生物力学因素。
使用经过验证的从C2至C7的颈椎有限元模型来研究颈椎干预中的生物力学因素。该有限元模型用于模拟三节段ACDF,采用椎间融合器,并从C4至C7进行带螺钉固定的颈椎前路钢板固定。然后将模型在T1椎体的下节点处进行约束,并在顶部椎体上施加生理载荷。在屈曲、伸展和侧方弯曲时施加2 Nm的纯力矩载荷。施加75 N的跟随轴向力以模拟颅骨重量和肌肉力量,采用标准程序进行施加。利用运动控制混合方案来理解脊柱生物力学的变化。
我们的颈椎有限元模型表明,在C4 - 7 ACDF术后,与C7 - T1的尾侧相邻节段相比,头侧相邻节段(C3 - 4)的活动度(ROM)增加更为显著(+90.38%),表明头侧相邻节段比尾侧相邻节段有更多的ROM代偿性增加,这可能使其更容易发生早期ASD。在C4 - 7 ACDF结构内,与C4 - 5和C5 - 6相比,C6 - 7节段在固定过程中固定最不牢固,与完整脊柱相比ROM减小最小(分别为-71.30% vs. -76.36%和-77.05%),这可能使C6 - 7节段发生假关节形成的风险更高。
使用经过验证的颈椎有限元模型对C4 - 7 ACDF结构进行生物力学分析表明,与C7 - T1相比,C3 - 4的ROM代偿性增加更多,并且在生理载荷下C6 - 7的固定最不牢固。这些发现可以帮助脊柱外科医生预测假关节形成和ASD风险较高的区域,从而制定相应策略来降低这些风险,并为患者提供适当的术前咨询。