Division of General Internal Medicine, Faculty of Medicine and Dentistry (McAlister), University of Alberta; The Alberta Strategy for Patient-Oriented Research Support Unit (McAlister, Dong, Youngson), Edmonton, Alta.; ICES (Chu, Wang, Quinn, Udell, de Mestral, van Walraven, Lee); University of Toronto (Chu, de Mestral, Ross); Department of Medicine, Divisions of General Internal Medicine and Palliative Care (Quinn), Sinai Health System, University of Toronto; Li Ka Shing Knowledge Institute (Verma, Razak), St. Michael's Hospital, Unity Health Toronto; Department of Medicine (Verma, Razak), University of Toronto; Institute of Health Policy, Management and Evaluation (Verma, Razak), Dalla Lana School of Public Health, University of Toronto; University Health Network (Udell, Ross, Lee); Department of Medicine (Neurology) (Yu), University of Toronto, Sunnybrook Health Sciences Centre, Toronto, Ont.; Division of Physical Medicine and Rehabilitation (Ho), Department of Medicine, Faculty of Medicine and Dentistry, University of Alberta, Edmonton, Alta.; Department of Surgery (de Mestral), Unity Health Toronto; Peter Munk Cardiac Center (Ross, Lee), Ted Rogers Centre for Heart Research, University of Toronto, Toronto, Ont.; Department of Medicine and School of Epidemiology and Public Health (van Walraven), University of Ottawa, Ottawa Hospital Research Institute, Ottawa, Ont.
CMAJ. 2022 May 16;194(19):E666-E673. doi: 10.1503/cmaj.220272.
The frequency of readmissions after COVID-19 hospitalizations is uncertain, as is whether current readmission prediction equations are useful for discharge risk stratification of COVID-19 survivors or for comparing among hospitals. We sought to determine the frequency and predictors of death or unplanned readmission after a COVID-19 hospital discharge.
We conducted a retrospective cohort study of all adults (≥ 18 yr) who were discharged alive from hospital after a nonpsychiatric, nonobstetric, acute care admission for COVID-19 between Jan. 1, 2020, and Sept. 30, 2021, in Alberta and Ontario.
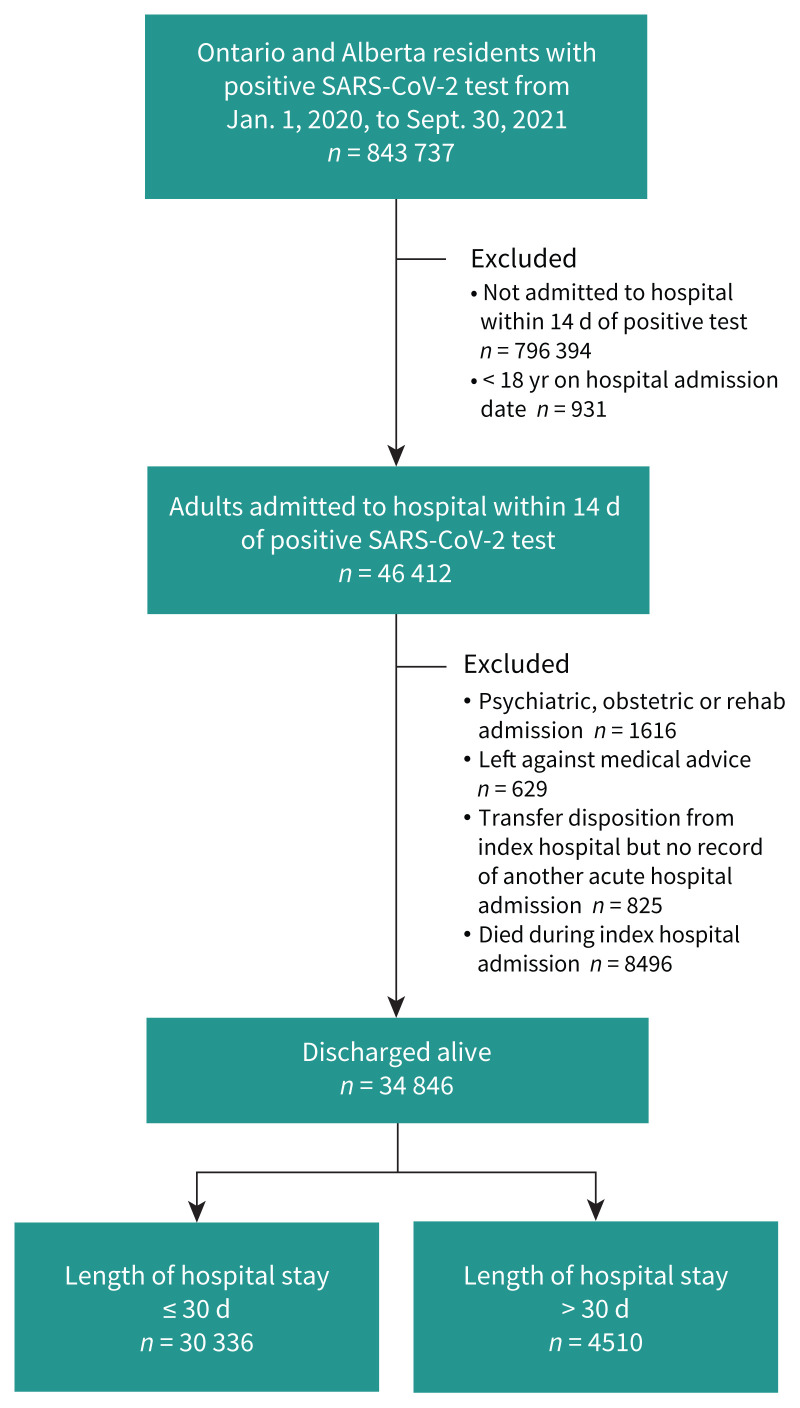
Of 843 737 individuals who tested positive for SARS-CoV-2 by reverse transcription polymerase chain reaction during the study period, 46 412 (5.5%) were adults admitted to hospital within 14 days of their positive test. Of these, 8496 died in hospital and 34 846 were discharged alive (30 336 discharged after an index admission of ≤ 30 d and 4510 discharged after an admission > 30 d). One in 9 discharged patients died or were readmitted within 30 days after discharge (3173 [10.5%] of those with stay ≤ 30 d and 579 [12.8%] of those with stay > 30 d). The LACE score (length of stay, acuity, Charlson Comorbidity Index and number of emergency visits in previous 6 months) for predicting urgent readmission or death within 30 days had a c-statistic of 0.60 in Alberta and 0.61 in Ontario; inclusion of sex, discharge locale, deprivation index and teaching hospital status in the model improved the c-statistic to 0.73.
Death or readmission after discharge from a COVID-19 hospitalization is common and had a similar frequency in Alberta and Ontario. Risk stratification and interinstitutional comparisons of outcomes after hospital admission for COVID-19 should include sex, discharge locale and socioeconomic measures, in addition to the LACE variables.
COVID-19 住院患者的再入院频率尚不确定,目前的再入院预测方程是否可用于 COVID-19 幸存者的出院风险分层或用于医院间比较也不确定。我们旨在确定 COVID-19 出院后死亡或非计划再入院的频率和预测因素。
我们对 2020 年 1 月 1 日至 2021 年 9 月 30 日期间,在艾伯塔省和安大略省因非精神科、非产科的急性 COVID-19 住院,出院时存活的所有成年人(≥18 岁)进行了回顾性队列研究。
在研究期间,通过逆转录聚合酶链反应检测到 SARS-CoV-2 阳性的 843737 人中,有 46412 人为在阳性检测后 14 天内住院的成年人。其中,8496 人在医院死亡,34846 人出院存活(30336 人在≤30d 的指数入院后出院,4510 人在>30d 的入院后出院)。出院后 30 天内,每 9 名出院患者中就有 1 人死亡或再入院(3173 人[10.5%]的住院时间≤30d,579 人[12.8%]的住院时间>30d)。在艾伯塔省和安大略省,用于预测 30 天内紧急再入院或死亡的 LACE 评分(住院时间、严重程度、Charlson 合并症指数和前 6 个月内急诊就诊次数)的 c 统计量分别为 0.60 和 0.61;在模型中纳入性别、出院地点、贫困指数和教学医院状态可将 c 统计量提高到 0.73。
COVID-19 住院后出院死亡或再入院很常见,在艾伯塔省和安大略省的发生率相似。COVID-19 住院患者的风险分层和出院后结果的医院间比较除了 LACE 变量外,还应包括性别、出院地点和社会经济措施。