Department of Medical Oncology and Clinical Research Unit, Institut Claudius Regaud, Toulouse, France
Department of Medicine, Centre Leon Berard, Lyon, France.
J Immunother Cancer. 2022 May;10(5). doi: 10.1136/jitc-2021-004076.
This phase 1b study (NCT02323191) evaluated the safety, antitumor activity, pharmacokinetics, and pharmacodynamics of colony-stimulating factor-1 receptor-blocking monoclonal antibody (mAb) emactuzumab in combination with the programmed cell death-1 ligand (PD-L1)-blocking mAb atezolizumab in patients with advanced solid tumors naïve or experienced for immune checkpoint blockers (ICBs).
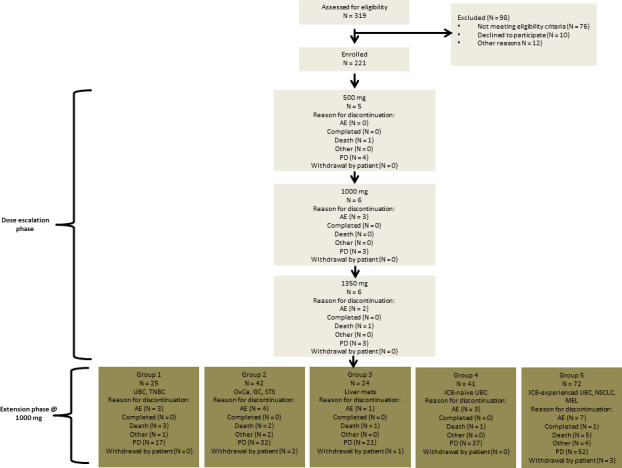
Emactuzumab (500-1350 mg flat) and atezolizumab (1200 mg flat) were administered intravenously every 3 weeks. Dose escalation of emactuzumab was conducted using the 3+3 design up to the maximum tolerated dose (MTD) or optimal biological dose (OBD). Extension cohorts to evaluate pharmacodynamics and clinical activity were conducted in metastatic ICB-naive urothelial bladder cancer (UBC) and ICB-pretreated melanoma (MEL), non-small cell lung cancer (NSCLC) and UBC patients.
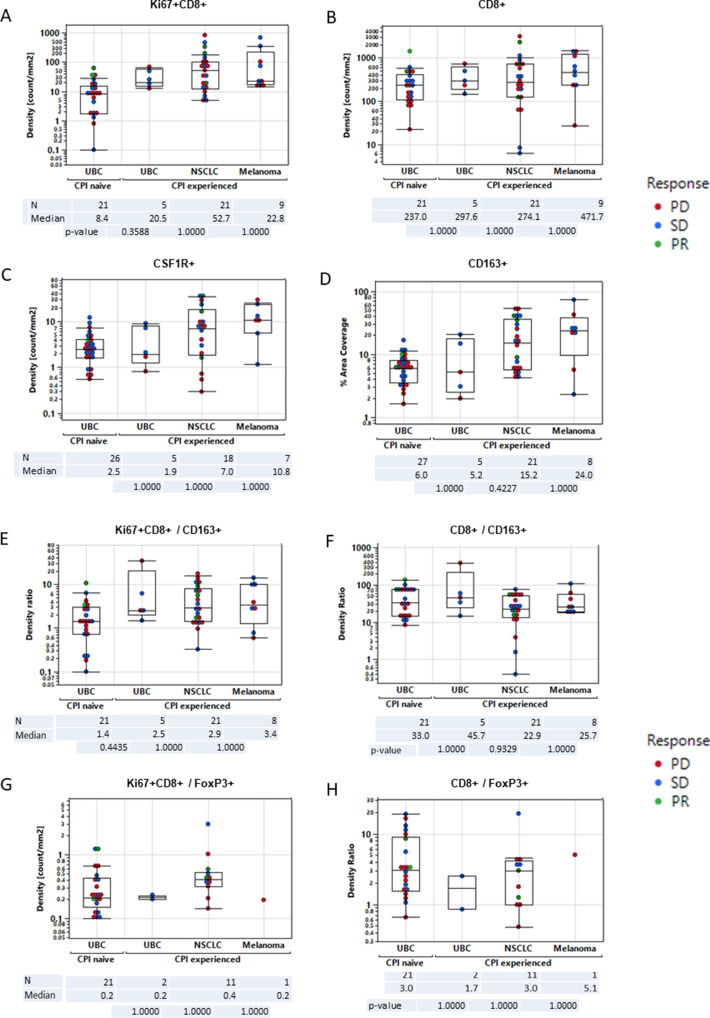
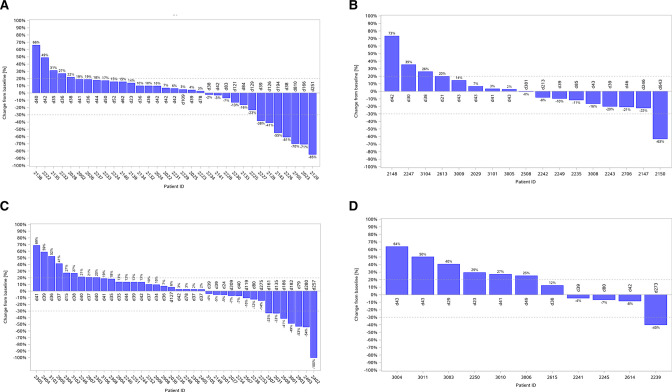
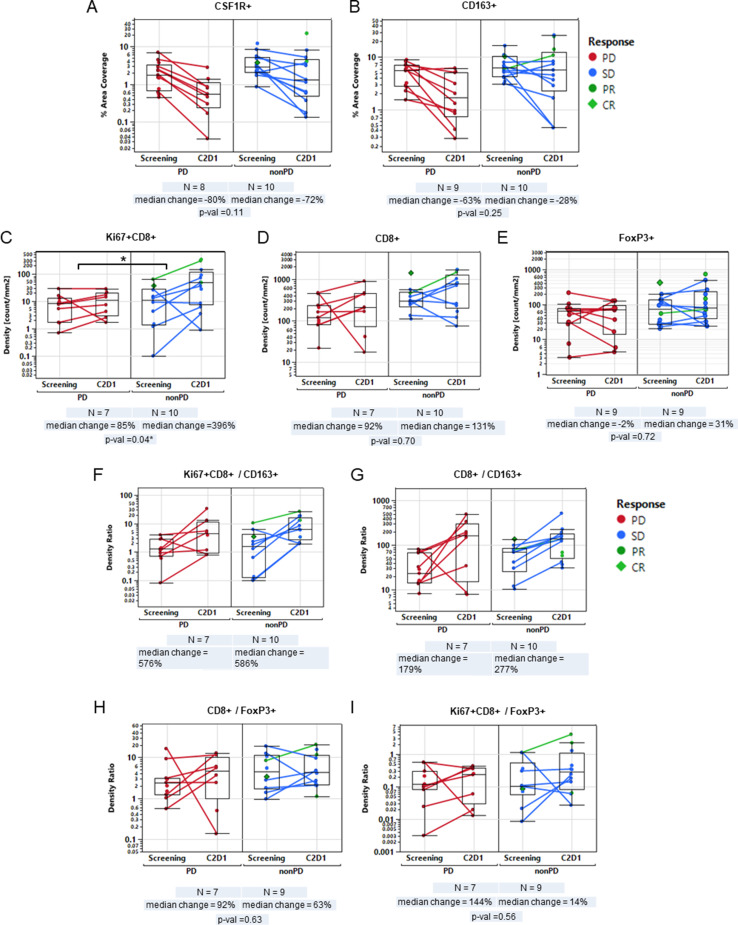
Overall, 221 patients were treated. No MTD was reached and the OBD was determined at 1000 mg of emactuzumab in combination with 1200 mg of atezolizumab. Grade ≥3 treatment-related adverse events occurred in 25 (11.3%) patients of which fatigue and rash were the most common (14 patients (6.3%) each). The confirmed objective response rate (ORR) was 9.8% for ICB-naïve UBC, 12.5% for ICB-experienced NSCLC, 8.3% for ICB-experienced UBC and 5.6% for ICB-experienced MEL patients, respectively. Tumor biopsy analyses demonstrated increased activated CD8 +tumor infiltrating T lymphocytes (TILs) associated with clinical benefit in ICB-naïve UBC patients and less tumor-associated macrophage (TAM) reduction in ICB-experienced compared with ICB-naïve patients.
Emactuzumab in combination with atezolizumab demonstrated a manageable safety profile with increased fatigue and skin rash over usual atezolizumab monotherapy. A considerable ORR was particularly seen in ICB-experienced NSCLC patients. Increase ofCD8 +TILs under therapy appeared to be associated with persistence of a TAM subpopulation.
这项 1b 期研究(NCT02323191)评估了集落刺激因子 1 受体阻断单克隆抗体(mAb)emactuzumab 联合程序性细胞死亡配体 1(PD-L1)阻断 mAb atezolizumab 在免疫检查点抑制剂(ICB)初治或经治的晚期实体瘤患者中的安全性、抗肿瘤活性、药代动力学和药效学。
emactuzumab(500-1350mg 平剂量)和 atezolizumab(1200mg 平剂量)每 3 周静脉输注一次。emactuzumab 的剂量递增采用 3+3 设计,直至最大耐受剂量(MTD)或最佳生物学剂量(OBD)。在转移性 ICB 初治的膀胱癌(UBC)和 ICB 预处理的黑色素瘤(MEL)、非小细胞肺癌(NSCLC)和 UBC 患者中进行了评估药效学和临床活性的扩展队列研究。
共有 221 名患者接受了治疗。未达到 MTD,确定 emactuzumab 联合 atezolizumab 的 OBD 为 1000mg。25 名(11.3%)患者发生≥3 级治疗相关不良事件,其中疲劳和皮疹最常见(各 14 例(6.3%))。ICB 初治 UBC 的确认客观缓解率(ORR)为 9.8%,ICB 经治 NSCLC 为 12.5%,ICB 经治 UBC 为 8.3%,ICB 经治 MEL 为 5.6%。肿瘤活检分析表明,在 ICB 初治 UBC 患者中,与临床获益相关的活化 CD8+肿瘤浸润 T 淋巴细胞(TIL)增加,与 ICB 初治患者相比,肿瘤相关巨噬细胞(TAM)减少。
emactuzumab 联合 atezolizumab 具有可管理的安全性,与常规 atezolizumab 单药治疗相比,疲劳和皮疹增加。在 ICB 经治 NSCLC 患者中,ORR 相当高。治疗期间 CD8+TIL 的增加似乎与 TAM 亚群的持续存在有关。