Swiss Tropical and Public Health Institute, Allschwil, Switzerland
University of Basel, Basel, Switzerland.
BMJ Glob Health. 2022 May;7(5). doi: 10.1136/bmjgh-2021-008346.
Children who receive prereferral rectal artesunate (RAS) require urgent referral to a health facility where appropriate treatment for severe malaria can be provided. However, the rapid improvement of a child's condition after RAS administration may influence a caregiver's decision to follow this recommendation. Currently, the evidence on the effect of RAS on referral completion is limited.
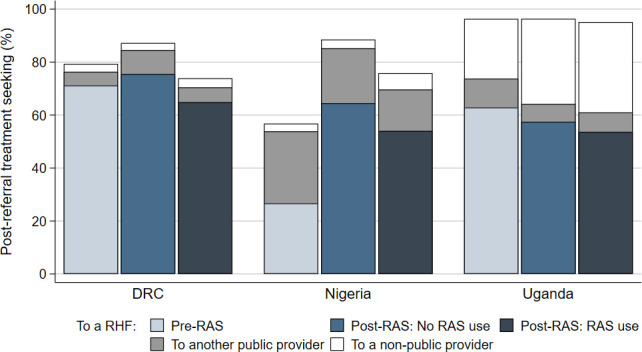
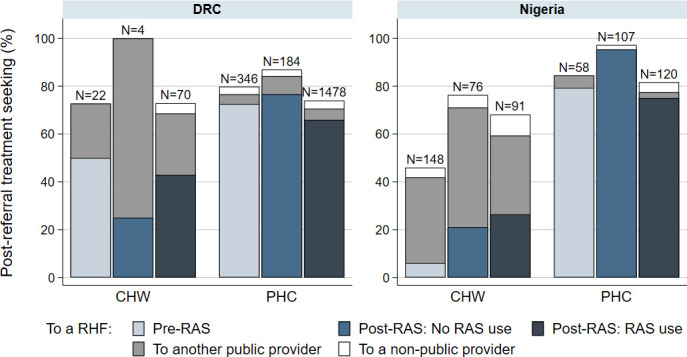
An observational study accompanied the roll-out of RAS in three malaria endemic settings in the Democratic Republic of the Congo (DRC), Nigeria and Uganda. Community health workers and primary health centres enrolled children under 5 years with suspected severe malaria before and after the roll-out of RAS. All children were followed up 28 days after enrolment to assess their treatment-seeking pathways.
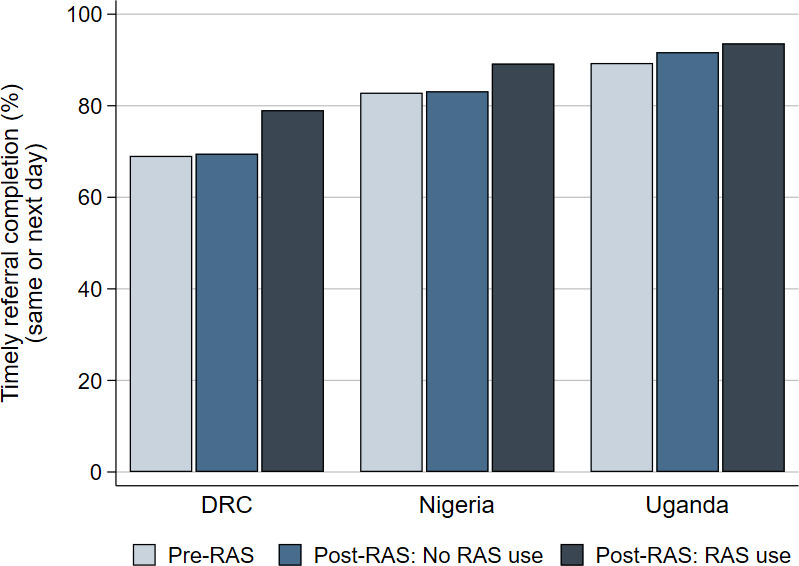
Referral completion was 67% (1408/2104) in DRC, 48% (287/600) in Nigeria and 58% (2170/3745) in Uganda. In DRC and Uganda, RAS users were less likely to complete referral than RAS non-users in the pre-roll-out phase (adjusted OR (aOR)=0.48, 95% CI 0.30 to 0.77 and aOR=0.72, 95% CI 0.58 to 0.88, respectively). Among children seeking care from a primary health centre in Nigeria, RAS users were less likely to complete referral compared with RAS non-users in the post-roll-out phase (aOR=0.18, 95% CI 0.05 to 0.71). In Uganda, among children who completed referral, RAS users were significantly more likely to complete referral on time than RAS non-users enrolled in the pre-roll-out phase (aOR=1.81, 95% CI 1.17 to 2.79).
The findings of this study raise legitimate concerns that the roll-out of RAS may lead to lower referral completion in children who were administered prereferral RAS. To ensure that community-based programmes are effectively implemented, barriers to referral completion need to be addressed at all levels. Alternative effective treatment options should be provided to children unable to complete referral.
NCT03568344; ClinicalTrials.gov.
接受预转诊直肠青蒿琥酯(RAS)的儿童需要紧急转诊至能提供重症疟疾适当治疗的医疗机构。然而,儿童在接受 RAS 治疗后病情迅速改善,可能会影响照护者对该建议的遵循意愿。目前,RAS 对转诊完成效果的证据有限。
在刚果民主共和国(DRC)、尼日利亚和乌干达三个疟疾流行地区开展 RAS 推广的同时,开展了一项观察性研究。社区卫生工作者和初级保健中心在 RAS 推广前后招募了疑似患有重症疟疾的 5 岁以下儿童。所有儿童在入组后 28 天进行随访,以评估他们的治疗寻求途径。
在 DRC、尼日利亚和乌干达,转诊完成率分别为 67%(1408/2104)、48%(287/600)和 58%(2170/3745)。在 DRC 和乌干达,RAS 使用者在推广前阶段比 RAS 非使用者更不可能完成转诊(调整后的 OR(aOR)=0.48,95%CI 0.30 至 0.77 和 aOR=0.72,95%CI 0.58 至 0.88)。在尼日利亚从初级保健中心寻求治疗的儿童中,RAS 使用者与 RAS 非使用者相比,在推广后阶段更不可能完成转诊(aOR=0.18,95%CI 0.05 至 0.71)。在乌干达,在完成转诊的儿童中,与在推广前阶段入组的 RAS 非使用者相比,RAS 使用者按时完成转诊的可能性显著更高(aOR=1.81,95%CI 1.17 至 2.79)。
这项研究的结果引发了合理的担忧,即 RAS 的推广可能会导致接受预转诊 RAS 的儿童的转诊完成率降低。为确保有效实施基于社区的方案,需要在各个层面解决转诊完成的障碍。对于无法完成转诊的儿童,应提供其他有效的替代治疗方案。
NCT03568344;ClinicalTrials.gov。