Swiss Tropical and Public Health Institute, Allschwil, Switzerland.
University of Basel, Basel, Switzerland.
BMC Med. 2022 Oct 11;20(1):343. doi: 10.1186/s12916-022-02541-8.
To prevent child deaths from severe malaria, early parenteral treatment is essential. Yet, in remote rural areas, accessing facilities offering parenteral antimalarials may be difficult. A randomised controlled trial found pre-referral treatment with rectal artesunate (RAS) to reduce deaths and disability in children who arrived at a referral facility with delay. This study examined the effectiveness of pre-referral RAS treatment implemented through routine procedures of established community-based health care systems.
An observational study accompanied the roll-out of RAS in the Democratic Republic of the Congo (DRC), Nigeria and Uganda. Children <5 years of age presenting to a community-based health provider with a positive malaria test and signs of severe malaria were enrolled and followed up during admission and after 28 days to assess their health status and treatment history. The primary outcome was death; covariates of interest included RAS use, referral completion, and post-referral treatment.
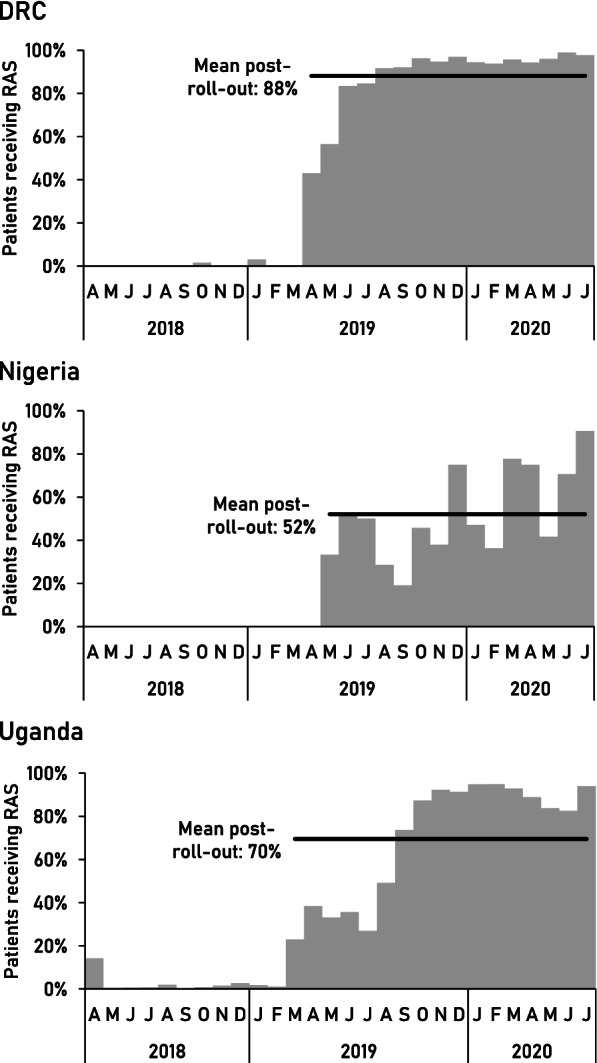
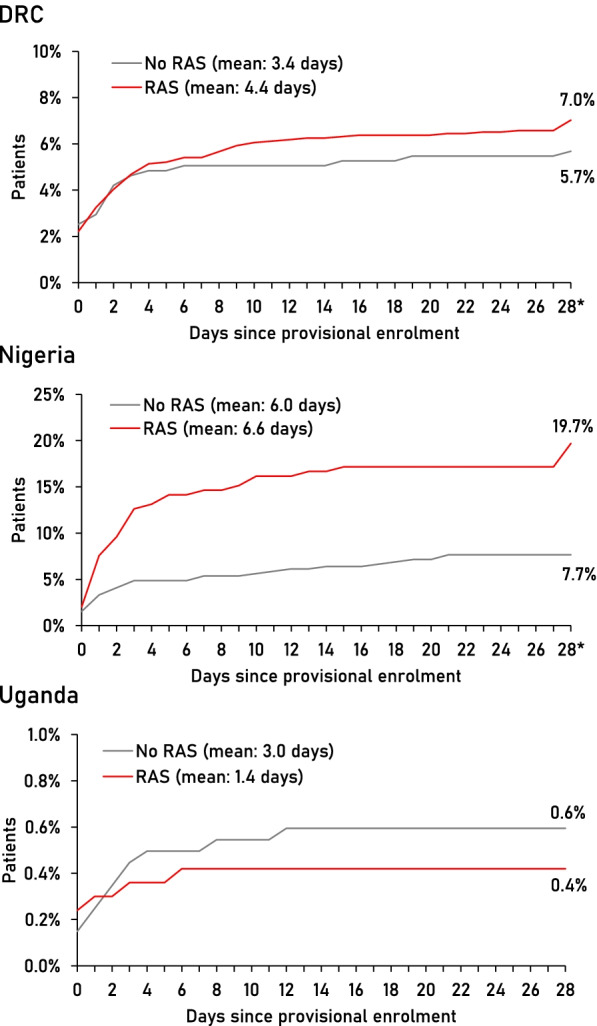
Post-roll-out, RAS was administered to 88% of patients in DRC, 52% in Nigeria, and 70% in Uganda. The overall case fatality rate (CFR) was 6.7% (135/2011) in DRC, 11.7% (69/589) in Nigeria, and 0.5% (19/3686) in Uganda; 13.8% (865/6286) of patients were sick on day 28. The CFR was higher after RAS roll-out in Nigeria (16.1 vs. 4.2%) and stable in DRC (6.7 vs. 6.6%) and Uganda (0.7 vs. 0.3%). In DRC and Nigeria, children receiving RAS were more likely to die than those not receiving RAS (aOR=3.06, 95% CI 1.35-6.92 and aOR=2.16, 95% CI 1.11-4.21, respectively). Only in Uganda, RAS users were less likely to be dead or sick at follow-up (aOR=0.60, 95% CI 0.45-0.79). Post-referral parenteral antimalarials plus oral artemisinin-based combination therapy (ACT), a proxy for appropriate post-referral treatment, was protective. However, in referral health facilities, ACT was not consistently administered after parenteral treatment (DRC 68.4%, Nigeria 0%, Uganda 70.9%).
Implemented at scale to the recommended target group, pre-referral RAS had no beneficial effect on child survival in three highly malaria-endemic settings. RAS is unlikely to reduce malaria deaths unless health system issues such as referral and quality of care at all levels are addressed.
The study is registered on ClinicalTrials.gov : NCT03568344.
为预防重症疟疾导致的儿童死亡,早期进行静脉治疗至关重要。然而,在偏远的农村地区,获得提供静脉抗疟药物的设施可能存在困难。一项随机对照试验发现,在转诊时使用直肠青蒿琥酯(RAS)进行预转诊治疗可降低因延迟到达转诊机构而出现的儿童的死亡和残疾风险。本研究评估了在既定的社区基础保健系统中通过常规程序实施预转诊 RAS 治疗的效果。
在刚果民主共和国(DRC)、尼日利亚和乌干达,一项观察性研究伴随着 RAS 的推出而进行。将年龄<5 岁、在社区保健提供者处接受过阳性疟疾检测且有严重疟疾体征的儿童纳入研究,并在住院期间和 28 天后进行随访,以评估其健康状况和治疗史。主要结局为死亡;感兴趣的协变量包括 RAS 使用、转诊完成情况和转诊后治疗。
在 RAS 推出后,DRC 有 88%的患者接受了 RAS 治疗,尼日利亚有 52%,乌干达有 70%。总体病死率(CFR)在 DRC 为 6.7%(135/2011),尼日利亚为 11.7%(69/589),乌干达为 0.5%(19/3686);13.8%(865/6286)的患者在第 28 天仍有症状。在尼日利亚,RAS 推出后 CFR 更高(16.1% vs. 4.2%),而在 DRC(6.7% vs. 6.6%)和乌干达(0.7% vs. 0.3%)则保持稳定。在 DRC 和尼日利亚,接受 RAS 治疗的儿童比未接受 RAS 治疗的儿童更有可能死亡(aOR=3.06,95%CI 1.35-6.92 和 aOR=2.16,95%CI 1.11-4.21)。仅在乌干达,RAS 使用者在随访时死亡或有症状的可能性较低(aOR=0.60,95%CI 0.45-0.79)。接受转诊后的静脉注射抗疟药物加口服青蒿琥酯-乙胺嘧啶复方疗法(ACT)是一种合适的转诊后治疗方法,具有保护作用。然而,在转诊卫生机构,ACT 在接受静脉注射治疗后并未持续给予(DRC 68.4%,尼日利亚 0%,乌干达 70.9%)。
在三个高度疟疾流行的地区,按照推荐的目标人群规模实施预转诊 RAS 治疗对儿童生存没有有益影响。除非解决了卫生系统问题,如转诊和各级医疗质量问题,否则 RAS 不太可能降低疟疾死亡率。
该研究在 ClinicalTrials.gov 上注册:NCT03568344。