Division of Maternal-Fetal Fetal Medicine, Prenatal Diagnosis Center, The International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, China.
Shanghai Key Laboratory of Embryo Original Diseases, Shanghai, China.
BMC Pregnancy Childbirth. 2022 May 18;22(1):417. doi: 10.1186/s12884-022-04754-4.
Due to the extensive development of assisted reproductive technology, the number of twin pregnancies has increased significantly over recent decades. Twin pregnancy is the most representative type of multiple pregnancies and is associated with high infant morbidity and mortality. Perinatal complications of twin pregnancy are also markedly increased compared with those of single pregnancy. Transabdominal selective reduction (SR) is a remedial intervention. This study aimed to research the adverse outcomes of transabdominal selective reduction of twin pregnancy and the correlation between the reduction week and pregnancy outcomes.
The purpose of this study was to examine the adverse outcomes of the transabdominal selective reduction of twin pregnancy and the correlation between the reduction week and pregnancy outcomes.
A retrospective cohort study of the transabdominal reduction of twin pregnancy was conducted in a single prenatal diagnosis medical centre from September 2012 to October 2020. According to chorionicity, women with twin pregnancies were divided into 2 groups: dichorionic (DC) twin pregnancies and monochorionic (MC) twin pregnancies. Women with DC twin pregnancies underwent potassium chloride reduction, and those with MC twin pregnancies underwent radiofrequency ablation (RFA). The reduction indications included pregnancy complications, foetal abnormalities, and maternal factors. The perinatal outcomes of different chorionic twins after reduction were analysed. Each foetus with an adverse outcome was included. The relative relationship between the reduction weeks and delivery weeks of twins was examined by correlation analysis.
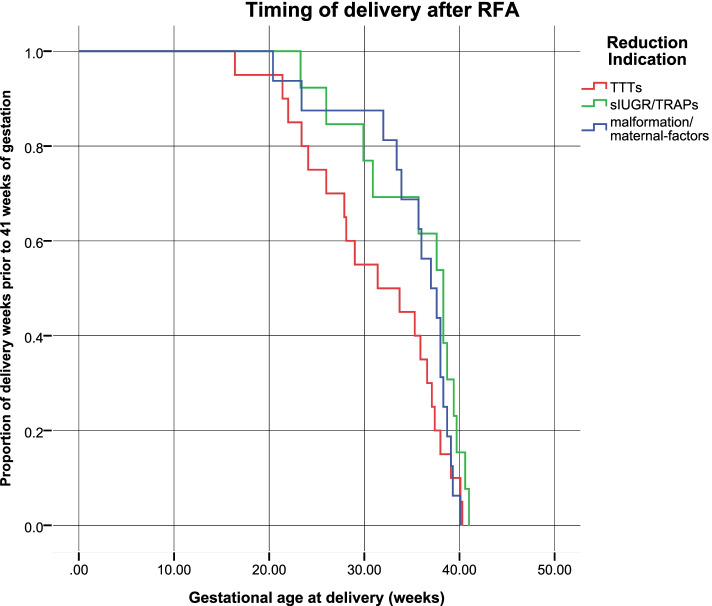
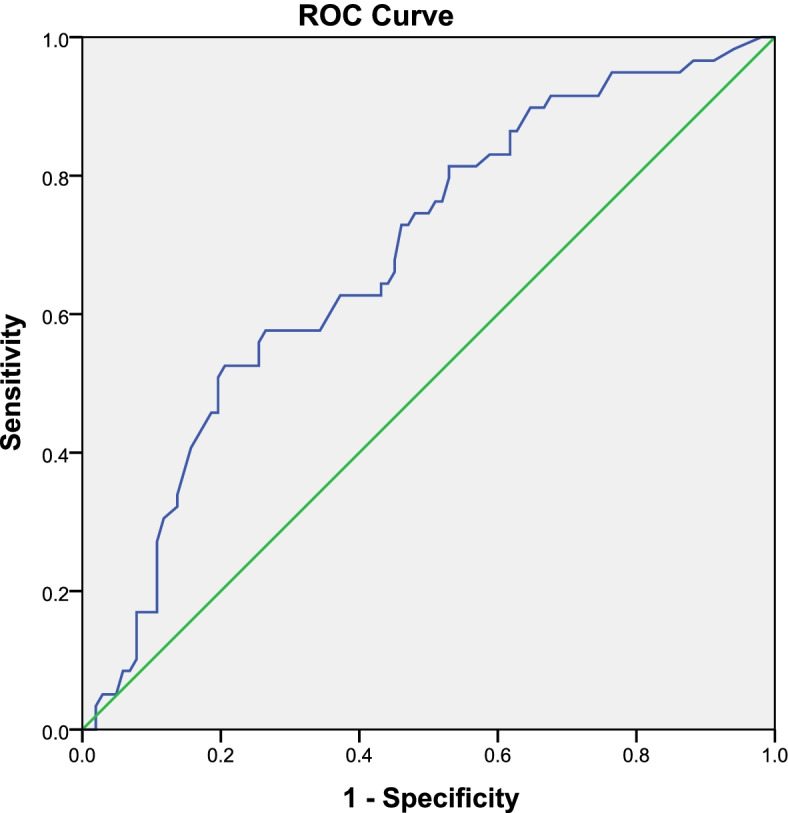
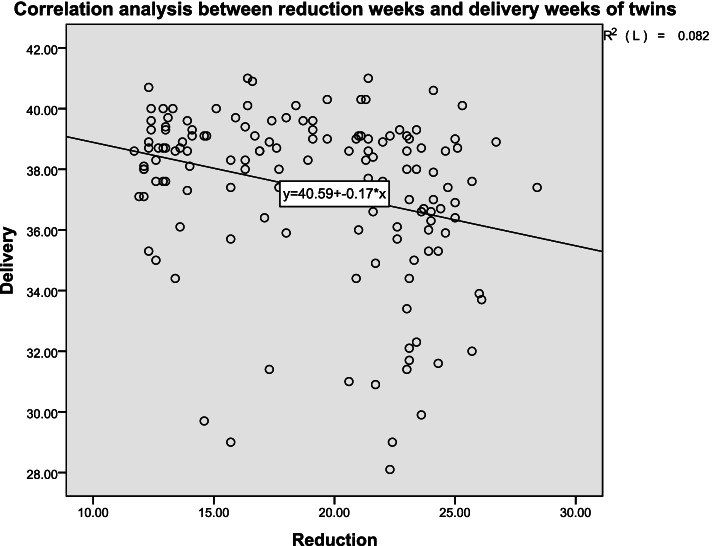
A total of 161 women were included in this study. A total of 112 women had DC twin pregnancies, and 49 women had MC twin pregnancies. Preterm delivery rates were significantly higher in the MC twin reduction group than in the DC twin reduction group prior to 37 weeks (53.1% vs. 29.5%, P = 0.004). The mean gestational age at delivery of the foetuses in the DC twin group that underwent SR was significantly older than that of those in the MC twin group that underwent SR (36.9 ± 4.0 vs. 33.5 ± 6.6 weeks, P = 0.001). The number of DC twins that underwent SR and were delivered after 37 weeks was obviously greater than that of the MC twins that underwent SR (70.5% vs. 46.9%, P = 0.004). The foetal survival rate was 95.5% in the DC twin reduction group and 77.6% in the MC twin reduction group. If the indication of TTTS was not included, there was no significant difference in the foetal survival rate of the DC and MC twin reduction groups (95.5% vs. 86.2%, P = 0.160). Cotwin death 1 week after reduction was greater in the MC group (6.1% vs. 0%, P = 0.027). Compared to other indications, this finding indicated that a significantly lower proportion of women remained undelivered after selective reduction with the indication of TTTS. There was a significant negative correlation between the reduction weeks and delivery weeks of the two groups (P < 0.01), and the best opportunity for reduction was before 22 weeks of gestation.
These findings highlighted an obviously negative correlation between the reduction week and delivery week. The transabdominal selective reduction of twin pregnancy should be considered for a lower rate of miscarriage or premature delivery if the reduction week takes place earlier in pregnancy. The rate of preterm delivery was the lowest when transabdominal selective reduction was completed before 22 weeks of gestation. Compared with other RFA indications, a higher rate of premature delivery was shown for MC twins with a reduction indication of TTTS. TTTS with sIUGR might be one of the reasons for the adverse outcomes of reduction for MC twin pregnancy.
由于辅助生殖技术的广泛发展,近几十年来双胞胎妊娠的数量显著增加。双胞胎妊娠是最具代表性的多胎妊娠类型,与婴儿发病率和死亡率高有关。与单胎妊娠相比,双胎妊娠的围产期并发症也明显增加。经腹选择性减胎术(SR)是一种补救干预措施。本研究旨在研究经腹选择性减胎术对双胞胎妊娠的不良后果以及减胎周数与妊娠结局的关系。
本研究的目的是研究经腹选择性减胎术对双胞胎妊娠的不良后果以及减胎周数与妊娠结局的关系。
对 2012 年 9 月至 2020 年 10 月在一家产前诊断医疗中心进行的经腹减胎术的回顾性队列研究。根据绒毛膜性,将双胎妊娠妇女分为 2 组:双绒毛膜(DC)双胎妊娠和单绒毛膜(MC)双胎妊娠。DC 双胎妊娠妇女行氯化钾减胎术,MC 双胎妊娠妇女行射频消融术(RFA)。减胎指征包括妊娠并发症、胎儿异常和母体因素。分析不同绒毛膜双胞胎减胎后的围产结局。每个出现不良结局的胎儿都被纳入研究。通过相关分析,检查两组双胞胎的减胎周数和分娩周数之间的相对关系。
本研究共纳入 161 名妇女。112 名妇女为 DC 双胎妊娠,49 名妇女为 MC 双胎妊娠。在 37 周之前,MC 双胎妊娠减胎组的早产率明显高于 DC 双胎妊娠减胎组(53.1%比 29.5%,P=0.004)。行 SR 的 DC 双胎妊娠组的平均分娩孕周明显长于行 SR 的 MC 双胎妊娠组(36.9±4.0 比 33.5±6.6 周,P=0.001)。行 SR 并在 37 周后分娩的 DC 双胎妊娠数量明显多于行 SR 的 MC 双胎妊娠(70.5%比 46.9%,P=0.004)。DC 双胎妊娠减胎组的胎儿存活率为 95.5%,MC 双胎妊娠减胎组为 77.6%。如果不包括 TTTS 的指征,DC 和 MC 双胎妊娠减胎组的胎儿存活率无显著差异(95.5%比 86.2%,P=0.160)。MC 组减胎后 1 周的双胎死亡发生率较高(6.1%比 0%,P=0.027)。与其他指征相比,这一发现表明 TTTS 指征的选择性减胎后,仍有较大比例的妇女未分娩。两组减胎周数与分娩周数呈显著负相关(P<0.01),最佳减胎时机为妊娠 22 周前。
这些发现强调了减胎周数与分娩周数之间明显的负相关。如果减胎周数较早,经腹选择性减胎术应考虑降低流产或早产的风险。在妊娠 22 周前完成经腹选择性减胎术时,早产率最低。与其他 RFA 指征相比,TTTS 减胎指征的 MC 双胞胎早产率较高。TTTS 合并 sIUGR 可能是 MC 双胞胎妊娠减胎不良结局的原因之一。