Keshtkarjahromi Marzieh, Abraham Danielle S, Gruber-Baldini Ann L, Schrader Katrina, Reich Stephen G, Savitt Joseph M, Von Coelln Rainer, Shulman Lisa M
MedStar Health, Internal Medicine Residency Program, Department of Medicine, Baltimore, MD, USA.
University of Pennsylvania, School of Medicine, Department of Neurology, Philadelphia, PA, USA.
Parkinsons Dis. 2022 May 9;2022:5535826. doi: 10.1155/2022/5535826. eCollection 2022.
The American Academy of Neurology Parkinson Disease (PD) quality measures include an annual diagnostic review.
To investigate the frequency and pattern of changes in diagnoses between PD and other causes of parkinsonism.
This prospective longitudinal cohort study included consented patients diagnosed with PD at least once and a minimum of two times at the Movement Disorders Center between 2002 and 2017. Movement disorder specialists confirmed and documented diagnoses at every visit. Longitudinal changes in diagnoses were identified across visits.
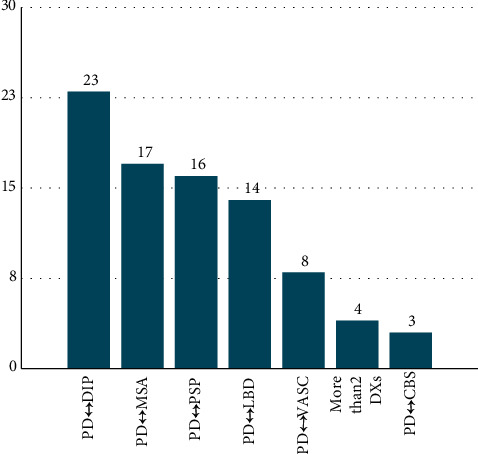
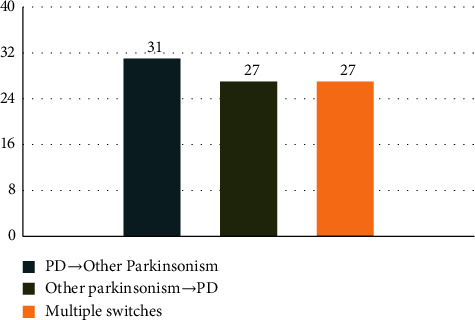
Of 1567 patients with parkinsonism, 174 had non-PD parkinsonism with no change over time. Of 1393 patients diagnosed with PD at least once, 94% ( = 1308) had no change of diagnosis over time and 6% ( = 85) had a change of diagnosis including PD ⟷ drug-induced parkinsonism (DIP) (27.1%), PD ⟷ multiple system atrophy (MSA) (20.0%), PD ⟷ progressive supranuclear palsy (PSP) (18.8%), PD ⟷ Lewy body dementia (DLB) (16.5%), PD⟷ vascular parkinsonism (9.4%), more than two diagnoses (4.7%), and PD ⟷ corticobasal syndrome (CBS) (3.5%). The direction of diagnostic switches was as follows: PD ⟶ other parkinsonism diseases (36.5%), other parkinsonism diseases ⟶ PD (31.8%), and 31.8% of multiple switches. There were no significant differences in duration of follow-up, age at first visit, gender, race, marital status, education, income, cognition, or employment between the stable and unstable groups. Diagnostic change was associated with greater PD severity and greater medical comorbidity.
Over a 15-year period, movement disorder specialists changed their clinical diagnosis of PD in 6% of patients. The most common diagnostic switches, to or from PD, were DIP, MSA, PSP, and DLB. This study describes routine clinical diagnostic patterns in the absence of pathologic confirmation. The presence of diverse diagnostic changes over time underscores the value of confirming PD diagnosis.
美国神经病学学会帕金森病(PD)质量指标包括年度诊断复查。
调查帕金森病与其他帕金森综合征病因之间诊断变化的频率和模式。
这项前瞻性纵向队列研究纳入了2002年至2017年间在运动障碍中心至少被诊断为帕金森病一次且至少两次的患者。运动障碍专家在每次就诊时确认并记录诊断。通过多次就诊确定诊断的纵向变化。
在1567例帕金森综合征患者中,174例患有非帕金森病性帕金森综合征,且病情未随时间变化。在至少被诊断为帕金森病一次的1393例患者中,94%(n = 1308)的诊断未随时间变化,6%(n = 85)的诊断发生了变化,包括帕金森病⟷药物性帕金森综合征(DIP)(27.1%)、帕金森病⟷多系统萎缩(MSA)(20.0%)、帕金森病⟷进行性核上性麻痹(PSP)(18.8%)、帕金森病⟷路易体痴呆(DLB)(16.5%)、帕金森病⟷血管性帕金森综合征(9.4%)、超过两种诊断(4.7%)以及帕金森病⟷皮质基底节综合征(CBS)(3.5%)。诊断转换的方向如下:帕金森病⟶其他帕金森综合征疾病(36.5%),其他帕金森综合征疾病⟶帕金森病(31.8%),以及31.8%的多次转换。稳定组和不稳定组在随访时间、首次就诊年龄、性别、种族、婚姻状况、教育程度、收入、认知或就业方面没有显著差异。诊断变化与帕金森病严重程度更高和医疗合并症更多相关。
在15年期间,运动障碍专家对6%的患者改变了帕金森病的临床诊断。与帕金森病之间最常见的诊断转换是DIP、MSA、PSP和DLB。本研究描述了在缺乏病理证实情况下的常规临床诊断模式。随着时间推移出现的多种诊断变化凸显了确认帕金森病诊断的价值。