Gerard Hilla, Iline Nicolas, Martel Hélène, Nguyen Karine, Richard Pascale, Donal Erwan, Eicher Jean-Christophe, Huttin Olivier, Selton-Suty Christine, Raud-Raynier Pascale, Jondeau Guillaume, Mansencal Nicolas, Sawka Caroline, Ader Flavie, Pruny Jean-François, Casalta Anne-Claire, Michel Nicolas, Donghi Valeria, Faivre Laurence, Giorgi Roch, Charron Philippe, Habib Gilbert
Cardiology Department, Assistance Publique Hopitaux de Marseille (APHM), La Timone Hospital, Marseille, France.
Assistance Publique Hopitaux de Marseille (APHM), Hop Timone, BioSTIC, Biostatistique et Technologies de l'Information et de la Communication, Marseille, France.
Front Cardiovasc Med. 2022 May 2;9:856160. doi: 10.3389/fcvm.2022.856160. eCollection 2022.
Whether left ventricular non-compaction (LVNC) bears a different prognosis than dilated cardiomyopathy (DCM) is still a matter of debate.
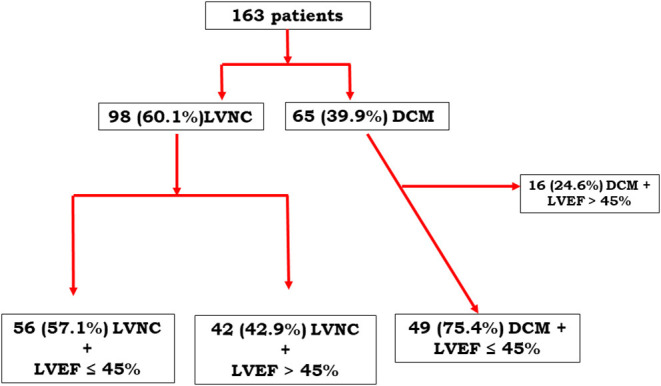
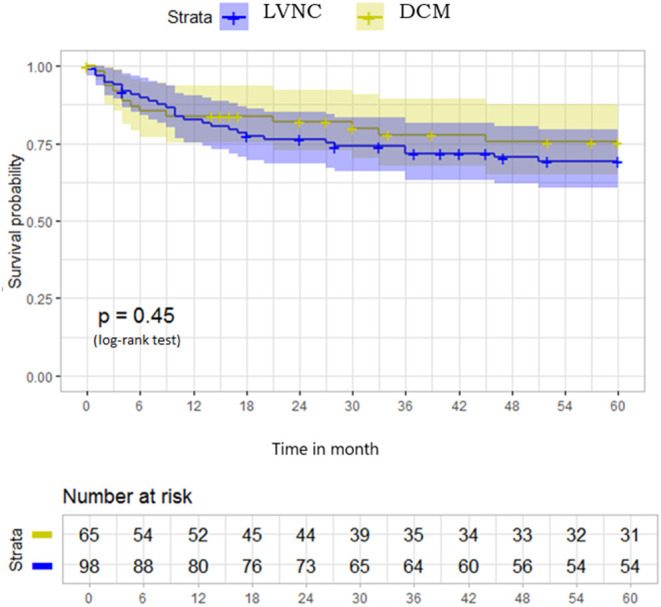
From a multicenter French prospective registry, we compared the outcomes of 98 patients with LVNC and 65 with DCM. The primary endpoint combined cardiovascular death, heart transplantation, and hospitalization for cardiovascular events. The two groups presented similar outcomes but different left ventricular ejection fractions (LVEF) (43.3% in LVNC vs. 35.95% in DCM, = 0.001). For this reason, a subgroup analysis was performed comparing only patients with LVEF 45%, including 56 with LVNC and 49 with DCM.
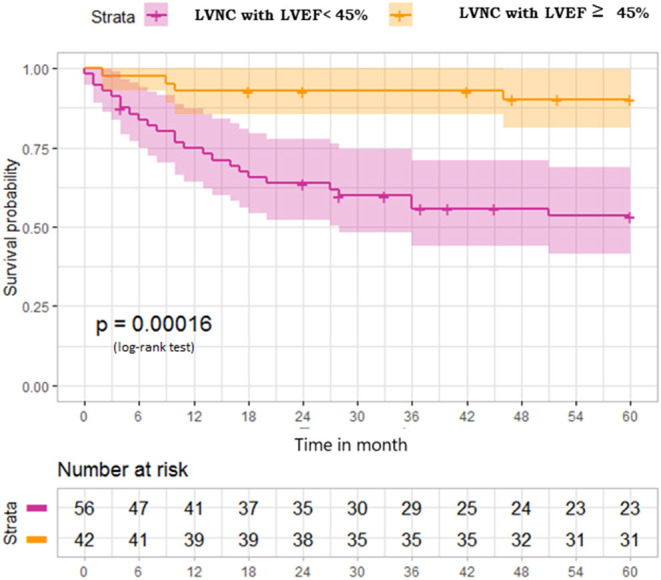
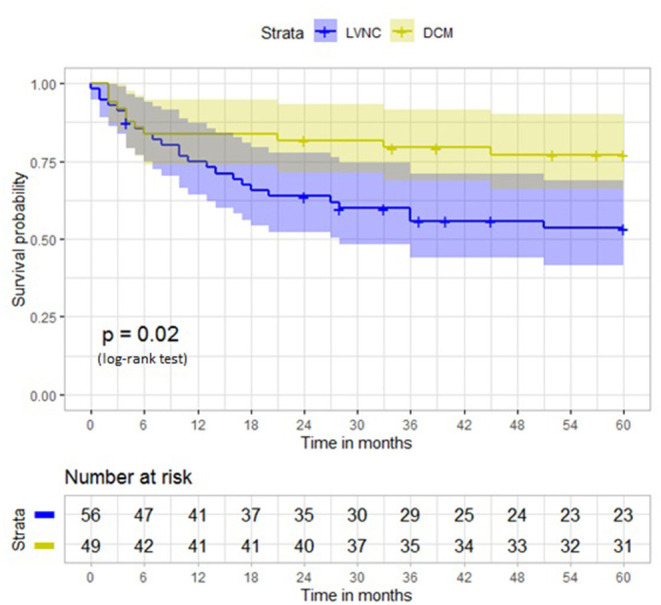
Among patients with LVEF 45%, at 5-year follow-up, the primary endpoint occurred in 33 (58.9%) among 56 patients with LVNC and 18 (36.7%) among 49 patients with DCM ( = 0.02). Hospitalization for heart failure (18 [32.14%] vs. 5 [10.20%], = 0.035) and heart transplantation were more frequent in the LVNC than in the DCM group. The incidences of rhythmic complications (24 [42.85%] vs. 12 [24.48%], = 0.17), embolic events, and cardiovascular death were similar between LVNC and DCM cases. Among the 42 patients with LVNC and LVEF > 45%, the primary endpoints occurred in only 4 (9.52%) patients, including 2 hospitalizations for heart failure and 3 rhythmic complications, but no embolic events.
In this prospective cohort, patients with LVNC who have left ventricular dysfunction present a poorer prognosis than DCM patients. Heart failure events were especially more frequent, but embolic events were not. Patients with LVNC and preserved ejection fraction present very few events in 5 years.
左心室心肌致密化不全(LVNC)与扩张型心肌病(DCM)的预后是否不同仍存在争议。
从法国一个多中心前瞻性登记处,我们比较了98例LVNC患者和65例DCM患者的结局。主要终点包括心血管死亡、心脏移植以及因心血管事件住院。两组呈现相似的结局,但左心室射血分数(LVEF)不同(LVNC组为43.3%,DCM组为35.95%,P = 0.001)。因此,进行了亚组分析,仅比较LVEF≤45%的患者,其中LVNC组56例,DCM组49例。
在LVEF≤45%的患者中,5年随访时,56例LVNC患者中有33例(58.9%)发生主要终点事件,49例DCM患者中有18例(36.7%)发生主要终点事件(P = 0.02)。LVNC组因心力衰竭住院(18例[32.14%] vs. 5例[10.20%],P = 0.035)和心脏移植比DCM组更频繁。LVNC组和DCM组在节律并发症(24例[42.85%] vs. 12例[24.48%],P = 0.17)、栓塞事件和心血管死亡的发生率方面相似。在42例LVEF>45%的LVNC患者中,仅4例(9.52%)发生主要终点事件,包括2例因心力衰竭住院和3例节律并发症,但无栓塞事件。
在这个前瞻性队列中,有左心室功能障碍的LVNC患者比DCM患者预后更差。心力衰竭事件尤其更频繁,但栓塞事件并非如此。LVEF保留的LVNC患者在5年内发生的事件很少。