Offord Centre for Child Studies, Psychiatry & Behavioural Neurosciences, McMaster University, Hamilton, ON, Canada.
Epidemiol Psychiatr Sci. 2022 May 19;31:e35. doi: 10.1017/S204579602200018X.
Prevalence estimates of child and youth mental disorder and mental health-related service contacts are needed for policy formulation, research, advocacy and resource allocation. Our aim is to compare prevalence estimates of child and youth mental disorder and mental health-related service contacts derived from general population survey data v. linked administrative health data.
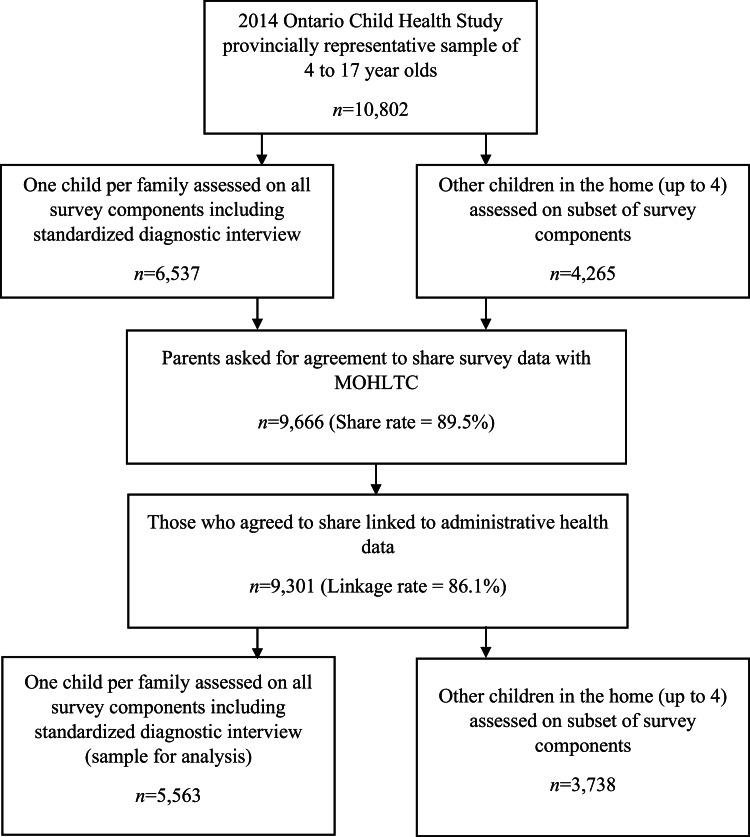
Provincially representative 2014 Ontario Child Health Study data were linked to administrative health records for 5563 children and youth aged 4-17 in Ontario. Emotional disorders (mood and anxiety) and attention-deficit/hyperactivity disorder were assessed using a standardised diagnostic interview in the survey and using diagnostic codes in administrative health data. Physician-based mental health-related service contacts were assessed using parent self-reports from the survey and administrative data related to mental health-related diagnostic codes. Prevalence estimates were calculated and compared based on one-sample z-tests and ratios of survey data to administrative data-based prevalence. Sensitivity, specificity and agreement between classifications were compared using κ. Prevalence estimates were calculated by age, sex and geography sub-groups and consistent group differences across data source were counted.
Disorder prevalence and service contact estimates were significantly higher in survey data in all cases, except for mood disorder. Ratios of survey data to administrative data-based prevalence varied, ranging from 0.80 (mood) to 11.01 (attention-deficit/hyperactivity disorder). Specificity was high (0.98-1.00), sensitivity was low (0.07-0.41) and agreement ranged from slight (κ = 0.13) to moderate (κ = 0.46). Out of 18 sub-group difference comparisons, half were non-significant in either data source. In the remaining nine comparisons, the only significant differences between groups that were consistent across data source were for sex-based differences (attention-deficit/hyperactivity disorder and service contacts). There were no consistent age- or geography-based differences in prevalence across data sources.
Our findings suggest that conclusions drawn about prevalence, service contacts and sub-group differences in these estimates are dependent on data source. Further research is needed to understand who and what is being captured by each source. Researchers should conduct data linkage where possible to access and compare multiple sources of information.
制定政策、开展研究、宣传倡导和资源配置都需要儿童和青少年精神障碍及与精神健康相关的服务利用的患病率估计值。本研究旨在比较来源于一般人群调查数据与链接的健康管理数据的儿童和青少年精神障碍及与精神健康相关的服务利用的患病率估计值。
对安大略省具有代表性的 2014 年儿童健康研究(Ontario Child Health Study)的数据进行链接,共纳入安大略省 4-17 岁的 5563 名儿童和青少年。使用标准化诊断访谈和健康管理数据中的诊断代码在调查中评估情绪障碍(心境和焦虑障碍)和注意缺陷多动障碍。使用调查中的父母自我报告和与精神健康相关的诊断代码相关的健康管理数据评估基于医生的与精神健康相关的服务利用情况。根据单一样本 z 检验和调查数据与健康管理数据为基础的患病率比值计算并比较患病率估计值。使用 κ 比较分类之间的灵敏度、特异度和一致性。按照年龄、性别和地理位置亚组计算患病率估计值,并计算在数据源中一致的亚组间差异的数量。
除心境障碍外,在所有情况下,调查数据中的障碍患病率和服务利用估计值都明显更高。调查数据与健康管理数据为基础的患病率比值不同,范围从 0.80(心境障碍)到 11.01(注意缺陷多动障碍)。特异度高(0.98-1.00),灵敏度低(0.07-0.41),一致性从轻度(κ=0.13)到中度(κ=0.46)不等。在 18 个亚组差异比较中,半数在两个数据源中均无统计学意义。在其余 9 个比较中,仅在数据源中一致的组间差异有统计学意义,为基于性别的差异(注意缺陷多动障碍和服务利用)。在数据源中,未观察到患病率在年龄或地理位置上的一致性差异。
我们的研究结果表明,这些估计值的患病率、服务利用和亚组差异的结论取决于数据源。需要进一步研究以了解每个来源捕获的内容和人群。研究人员应尽可能进行数据链接,以获取和比较多个来源的信息。