Dhaliwal Manpreet, Tyagi Rahul, Malhotra Pooja, Barman Prabal, Loganathan Sathish Kumar, Sharma Jyoti, Sharma Kaushal, Mondal Sanjib, Rawat Amit, Singh Surjit
Allergy and Immunology Unit, Department of Pediatrics, Advanced Pediatrics Center, Postgraduate Institute of Medical Education and Research, Chandigarh, India.
Front Pediatr. 2022 May 5;10:790273. doi: 10.3389/fped.2022.790273. eCollection 2022.
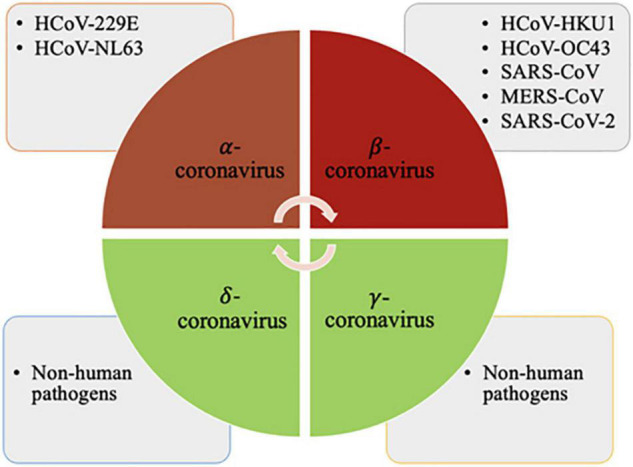
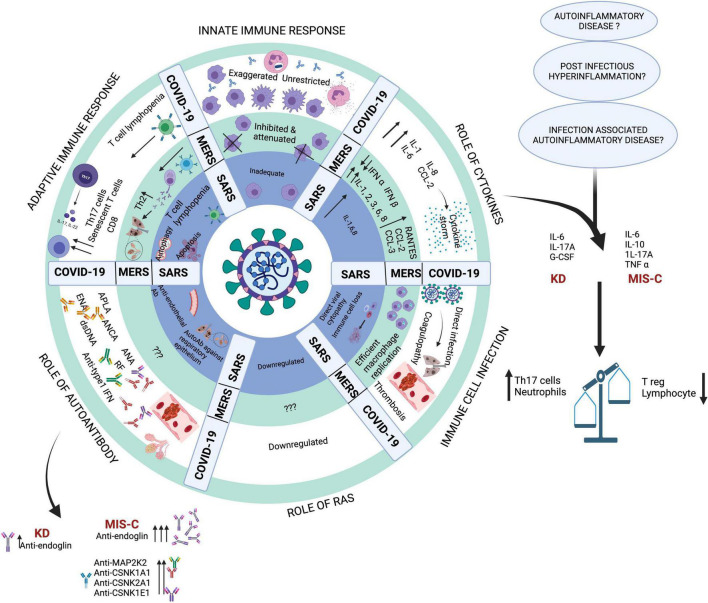
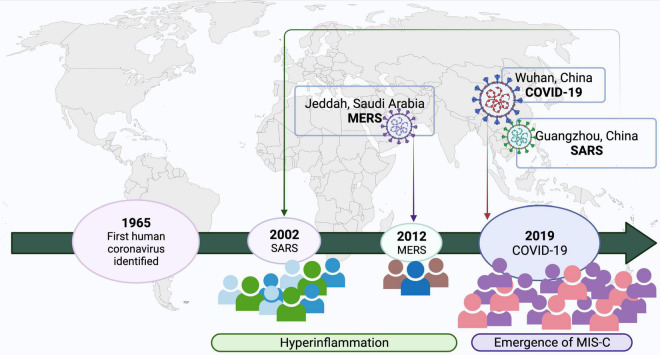
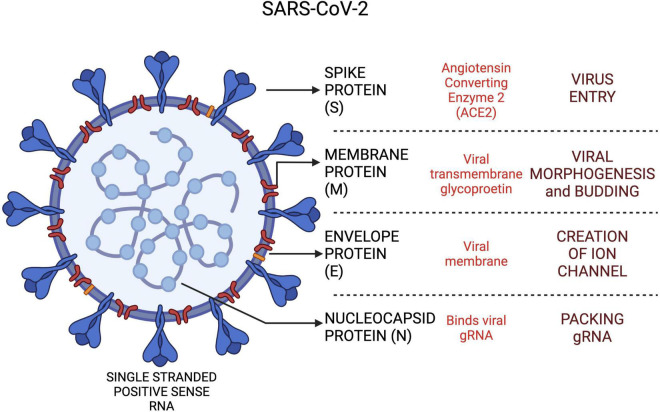
Coronaviruses have led to three major outbreaks to date-Severe Acute Respiratory Syndrome (SARS; 2002), Middle East Respiratory Syndrome (MERS; 2012) and the ongoing pandemic, Coronavirus Disease (COVID-19; 2019). Coronavirus infections are usually mild in children. However, a few children with MERS had presented with a severe phenotype in the acute phase resulting in progressive pneumonic changes with increasing oxygen dependency and acute respiratory distress requiring ventilatory support. A subset of children with a history of SARS-CoV-2 infection develops a multisystem hyper-inflammatory phenotype known as Multisystem Inflammatory Syndrome in Children (MIS-C). This syndrome occurs 4-6 weeks after infection with SARS-CoV-2 and has been reported more often from areas with high community transmission. Children with MIS-C present with high fever and often have involvement of cardiovascular, gastrointestinal and hematologic systems leading to multiorgan failure. This is accompanied by elevation of pro-inflammatory cytokines such as IL-6 and IL-10. MIS-C has several similarities with Kawasaki disease (KD) considering children with both conditions present with fever, rash, conjunctival injection, mucosal symptoms and swelling of hands and feet. For reasons that are still not clear, both KD and MIS-C were not reported during the SARS-CoV and MERS-CoV outbreaks. As SARS-CoV-2 differs from SARS-CoV by 19.5% and MERS by 50% in terms of sequence identity, differences in genomic and proteomic profiles may explain the varied disease immunopathology and host responses. Left untreated, MIS-C may lead to severe abdominal pain, ventricular dysfunction and shock. Immunological investigations reveal reduced numbers of follicular B cells, increased numbers of terminally differentiated CD4T lymphocytes, and decreased IL-17A. There is still ambiguity about the clinical and immunologic risk factors that predispose some children to development of MIS-C while sparing others. Host-pathogen interactions in SARS, MERS and COVID-19 are likely to play a crucial role in the clinical phenotypes that manifest. This narrative review focuses on the immunological basis for development of MIS-C syndrome in the ongoing SARS-CoV-2 pandemic. To the best of our knowledge, these aspects have not been reviewed before.
冠状病毒迄今为止已引发了三次重大疫情——严重急性呼吸综合征(SARS;2002年)、中东呼吸综合征(MERS;2012年)以及当前的大流行疾病冠状病毒病(COVID-19;2019年)。冠状病毒感染在儿童中通常较为轻微。然而,一些感染MERS的儿童在急性期表现出严重的症状,导致进行性肺部病变,氧依赖增加,并出现需要通气支持的急性呼吸窘迫。一部分有SARS-CoV-2感染史的儿童会出现一种多系统高炎症表型,称为儿童多系统炎症综合征(MIS-C)。这种综合征在感染SARS-CoV-2后4至6周出现,在社区传播率高的地区报告更为频繁。患有MIS-C的儿童表现为高热,且常累及心血管、胃肠道和血液系统,导致多器官功能衰竭。这伴随着促炎细胞因子如IL-6和IL-10的升高。考虑到患有这两种疾病的儿童都有发热、皮疹、结膜充血、黏膜症状以及手脚肿胀,MIS-C与川崎病(KD)有一些相似之处。由于尚不清楚的原因,在SARS-CoV和MERS-CoV疫情期间均未报告KD和MIS-C。由于SARS-CoV-2与SARS-CoV的序列同一性相差19.5%,与MERS相差50%,基因组和蛋白质组图谱的差异可能解释了不同的疾病免疫病理学和宿主反应。若不治疗,MIS-C可能导致严重腹痛、心室功能障碍和休克。免疫学研究显示滤泡B细胞数量减少、终末分化CD4T淋巴细胞数量增加以及IL-17A减少。对于使一些儿童易患MIS-C而另一些儿童幸免的临床和免疫危险因素仍存在不确定性。SARS、MERS和COVID-19中的宿主-病原体相互作用可能在表现出的临床表型中起关键作用。这篇叙述性综述聚焦于当前SARS-CoV-2大流行中MIS-C综合征发生发展的免疫学基础。据我们所知,这些方面此前尚未被综述过。